

Use of consensus clustering to identify subtypes of clinical early-stage non-small cell lung cancer and its association with lymph node metastasis
- PMID: 40238041
- PMCID: PMC12003233
- DOI: 10.1007/s12672-025-02148-4
Use of consensus clustering to identify subtypes of clinical early-stage non-small cell lung cancer and its association with lymph node metastasis
Abstract
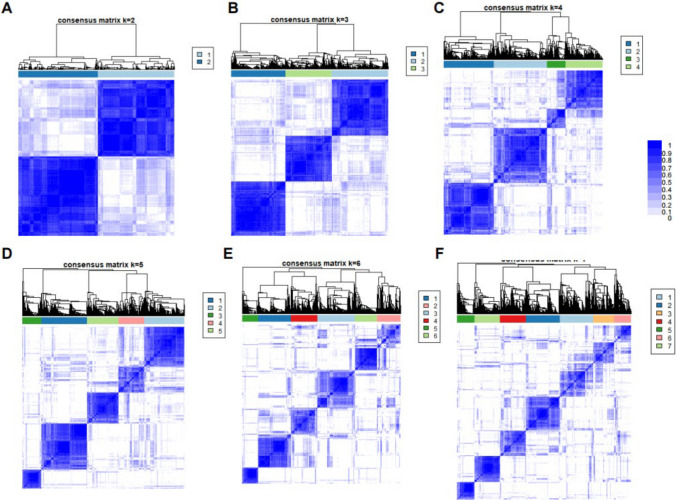
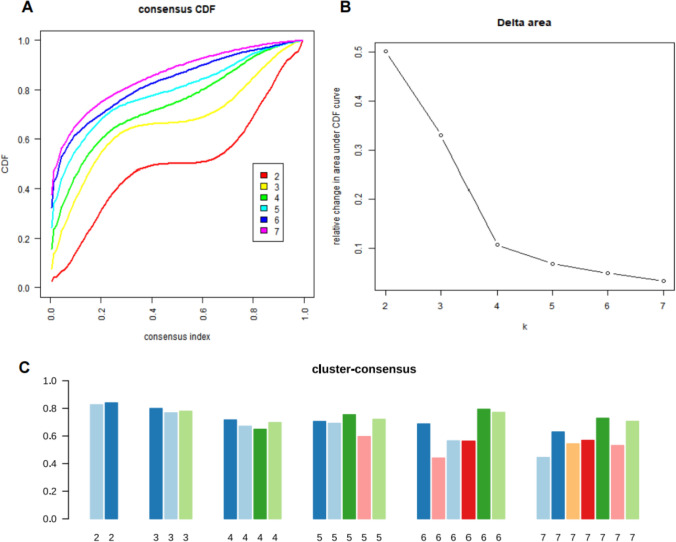
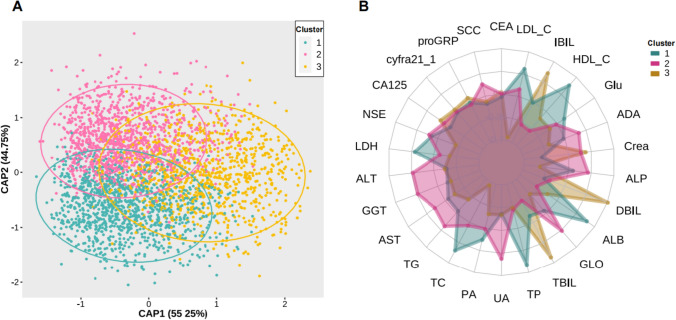
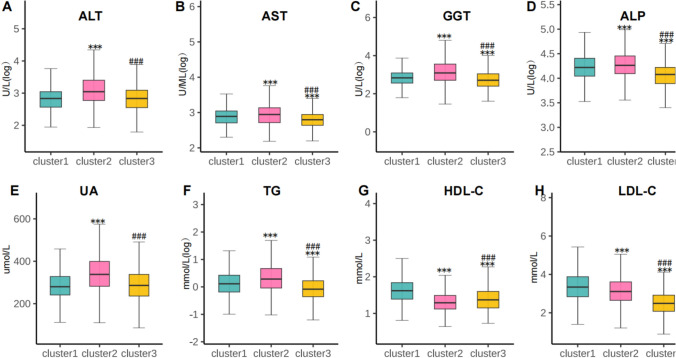
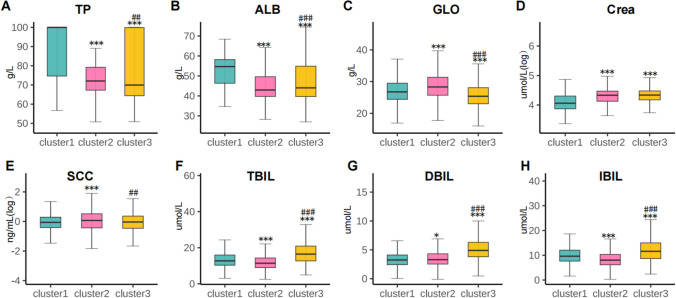
Limited studies have investigated the metabolic heterogeneity of patients with clinical early-stage non-small cell lung cancer (NSCLC). Consensus clustering analysis has the potential to reveal distinct metabolic subgroups within clinical early-stage NSCLC patients. A total of 3324 clinical early-stage NSCLC patients who underwent surgery were included in this comprehensive evaluation. The evaluation encompassed 26 serum assessments related to metabolism and histopathological examination of the lymph nodes. By utilizing consensus clustering analysis, three clusters were identified based on various measurements, including blood glucose levels, blood uric acid, blood lipids, renal and liver function, and tumor markers. The differences in characteristics and lymph node metastasis (LNM) prevalence between the clusters were investigated and compared. The patients were classified into three distinct clusters that exhibited different patterns defined by the highest or lowest levels of metabolic feature variables. NSCLC cluster 1 had the lowest rates of LNM, while cluster 3 showed a significantly higher prevalence of LNM (1.6-fold increase, 95% CI: 1.21, 2.13) compared to cluster 1. Moreover, cluster 2 had the highest odds ratio (OR) of 1.78 (95% CI: 1.37, 2.33) for LNM prevalence. In subsequent sensitivity analysis, metabolic heterogeneity was observed among patients with a tumor measuring less than 2 cm in the long axis, along with similar differences in the prevalence of lymph node metastasis. This present study successfully categorized clinical early-stage NSCLC into three distinct subgroups, each with unique characteristics that reflect metabolic heterogeneity and significant disparities in the prevalence of LNM. Such an approach holds potential implications for clinical early-stage interventions targeting risk factors.
Keywords: Consensus clustering analysis; LNM; Metabolic heterogeneity; NSCLC.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: This study was approved by the ethics committee of the Affiliated Hospital of Qingdao University. Informed consent was obtained from all patients, and the reported investigations were carried out in accordance with the principles of the Declaration of Helsinki as revised in 2008. Competing interests: The authors declare no competing interests.
Figures
References
-
- Rami-Porta R, Nishimura KK, Giroux DJ, Detterbeck F, Cardillo G, Edwards JG, Fong KM, Giuliani M, Huang J, Kernstine KH Sr, et al. The international association for the study of lung cancer lung cancer staging project: proposals for revision of the TNM stage groups in the forthcoming (ninth) edition of the TNM classification for lung cancer. J Thorac Oncol. 2024;19(7):1007–27. - DOI - PubMed
-
- Schuurbiers OC, Meijer TW, Kaanders JH, Looijen-Salamon MG, de Geus-Oei LF, van der Drift MA, van der Heijden EH, Oyen WJ, Visser EP, Span PN, et al. Glucose metabolism in NSCLC is histology-specific and diverges the prognostic potential of 18FDG-PET for adenocarcinoma and squamous cell carcinoma. J Thorac Oncol. 2014;9(10):1485–93. - DOI - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources