

Regional Citrate Anticoagulation Versus Systemic Heparin in Continuous Kidney Replacement Therapy: Examining the Role of Evidence in Health Technology Assessment
- PMID: 40238058
- PMCID: PMC12085351
- DOI: 10.1007/s12325-025-03186-8
Regional Citrate Anticoagulation Versus Systemic Heparin in Continuous Kidney Replacement Therapy: Examining the Role of Evidence in Health Technology Assessment
Abstract
Introduction: Continuous kidney replacement therapy (CKRT) is an established treatment supporting kidney function in patients with severe acute kidney disease. Systemic heparin and regional citrate anticoagulation (RCA) are the main anticoagulation strategies to prevent dialysis filter loss due to clotting, a complication of all KRT, including CKRT. The present study aims to comprehensively compare two anticoagulation strategies by collecting available clinical and economic evidence for an adult population under CKRT through a systematic literature review and meta-analysis.
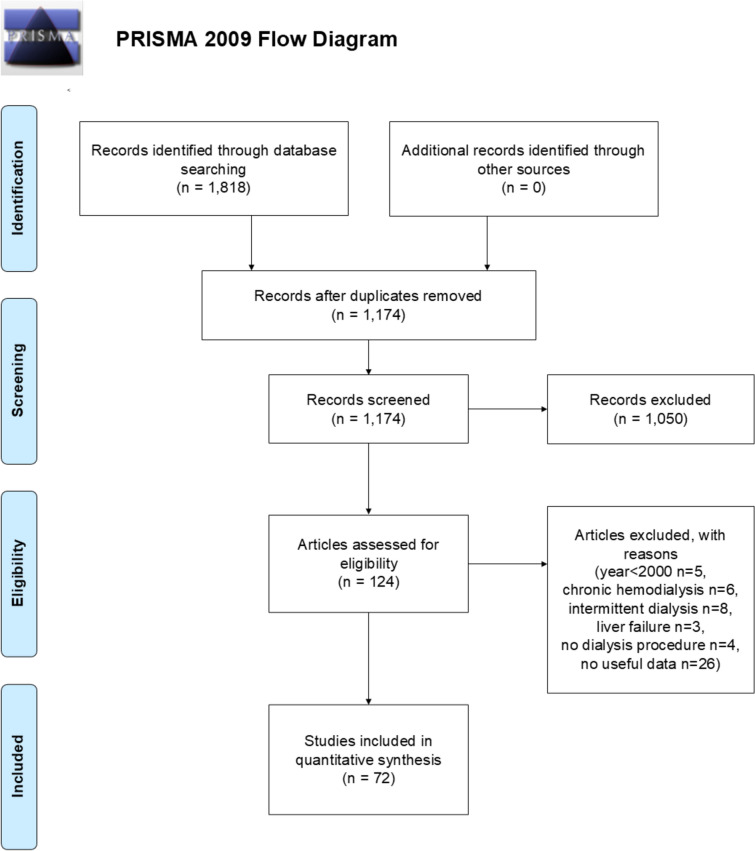
Methods: Randomized controlled trials, prospective/retrospective observational studies and economic analyses, involving systemic heparin or RCA, were searched through PubMed and Web of Science databases. Extracted data focused on clinical parameters, adverse events and cost items. Meta-analyses were conducted on data points with numeric outcomes to compare the two anticoagulation techniques. An evaluation of the quality of the evidence was also conducted using the GRADE system.
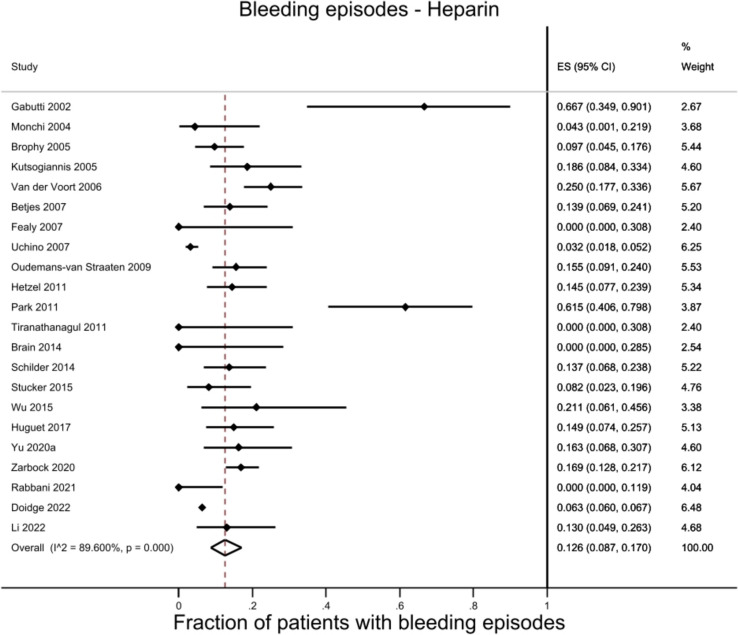
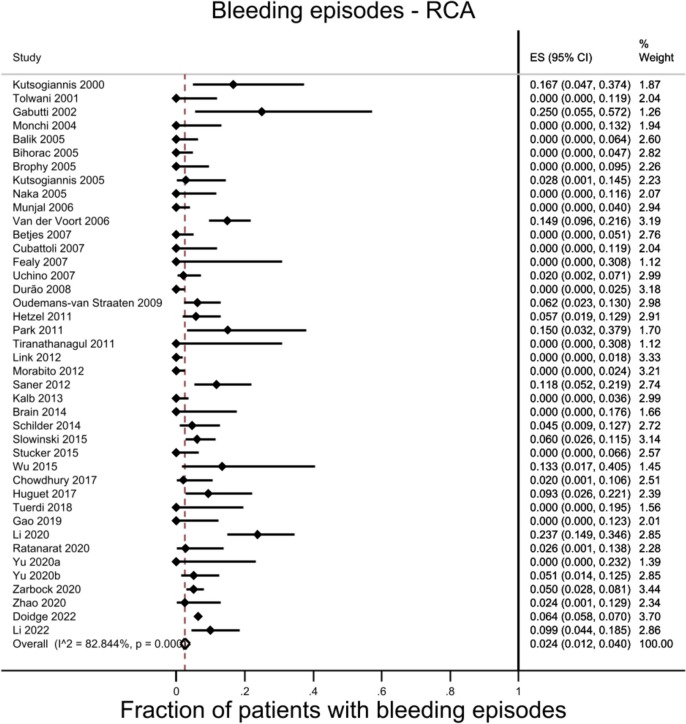
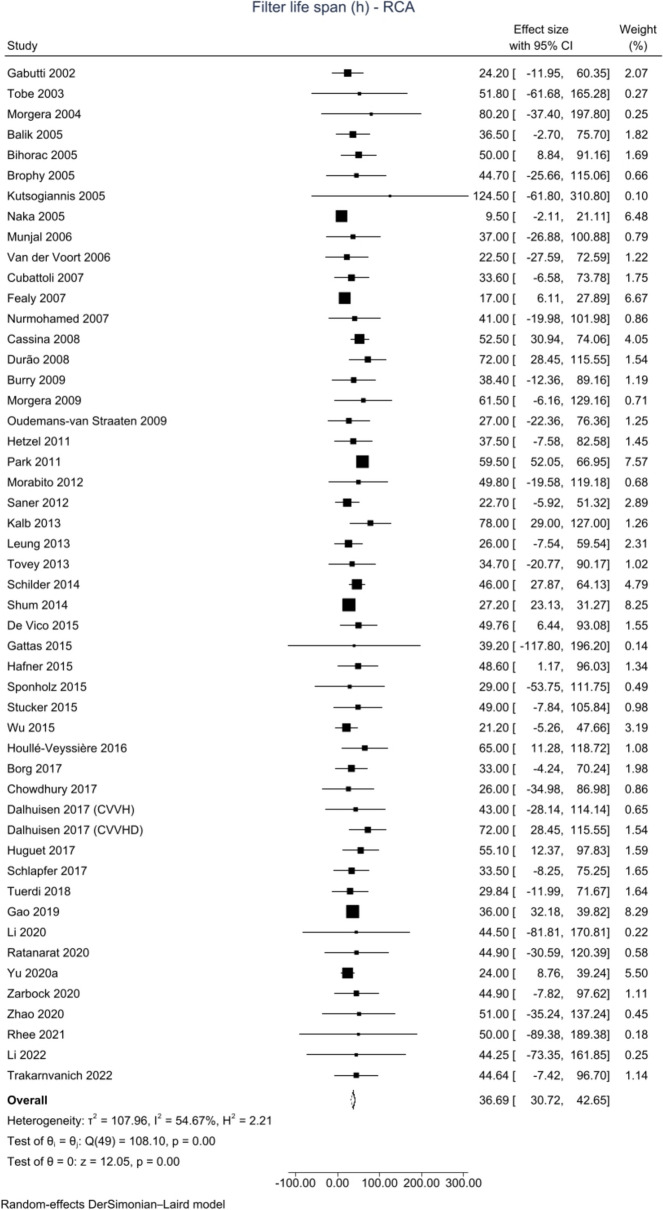
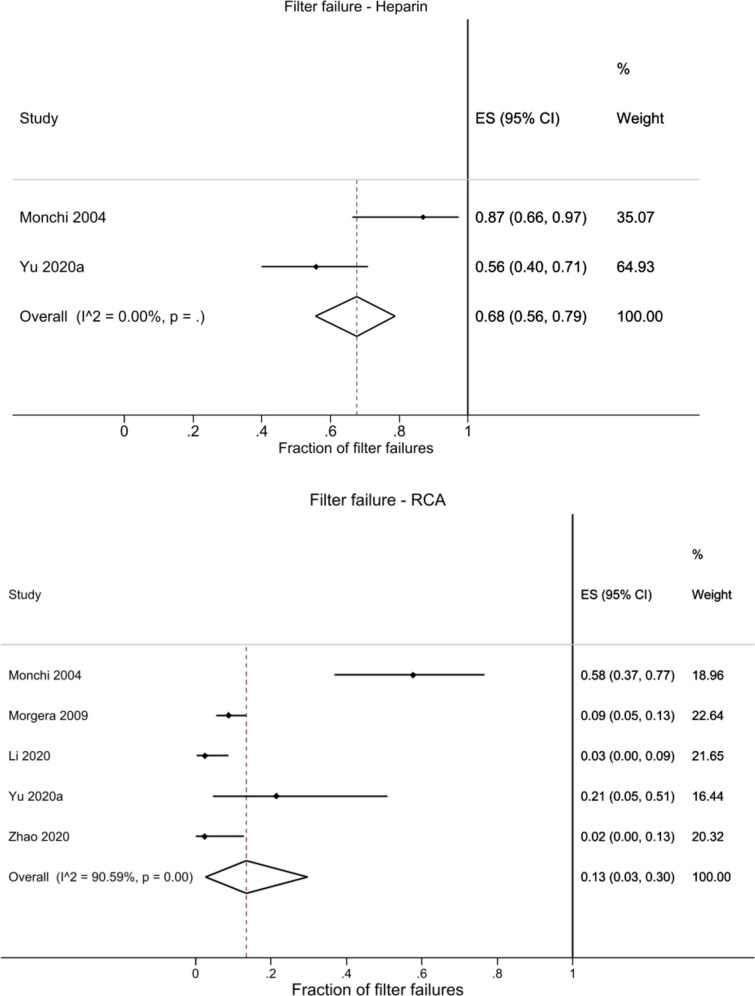
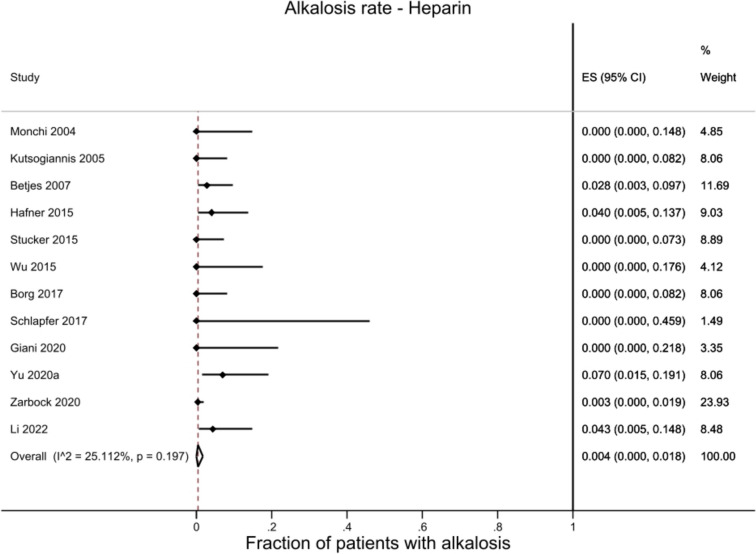
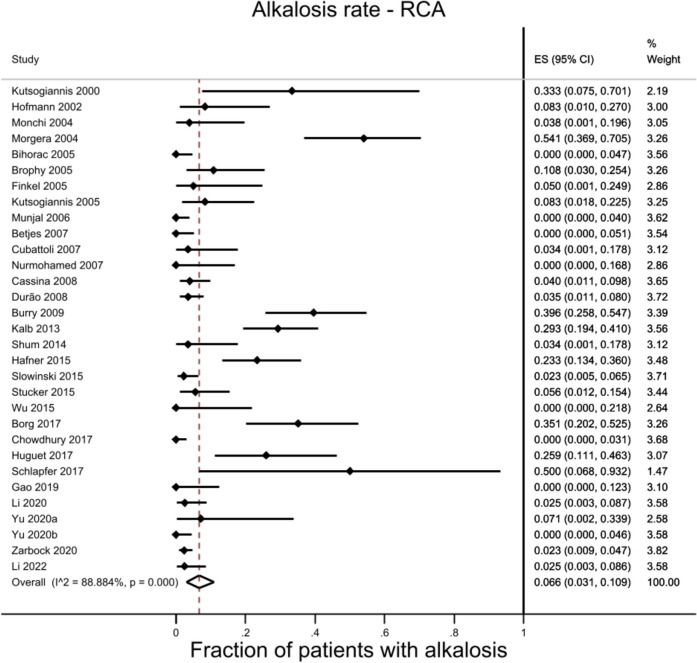
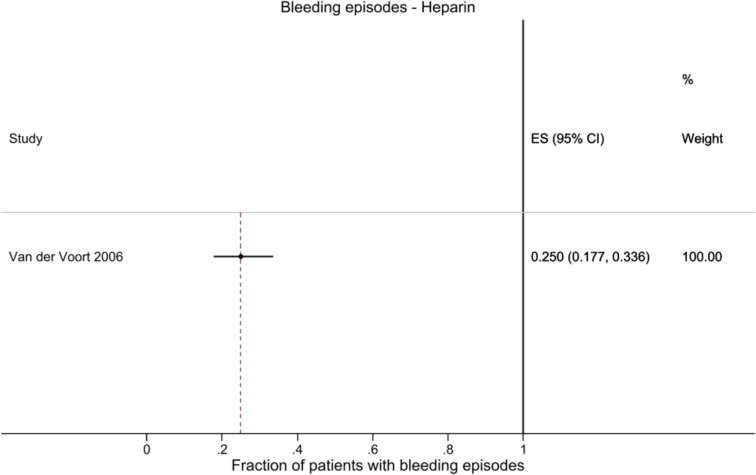
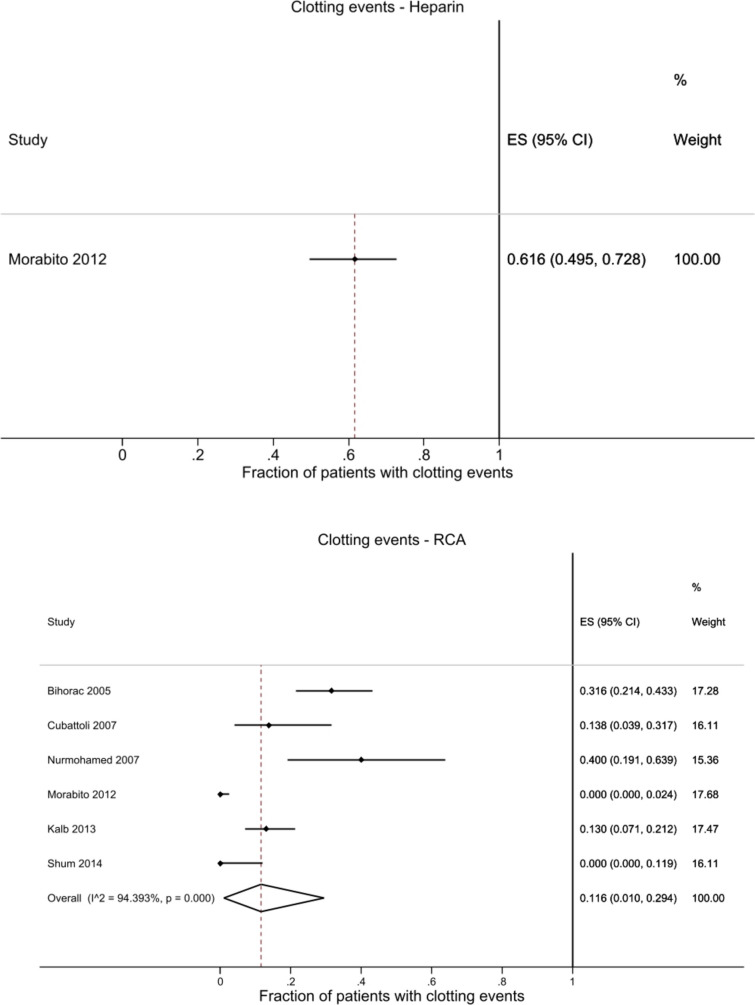
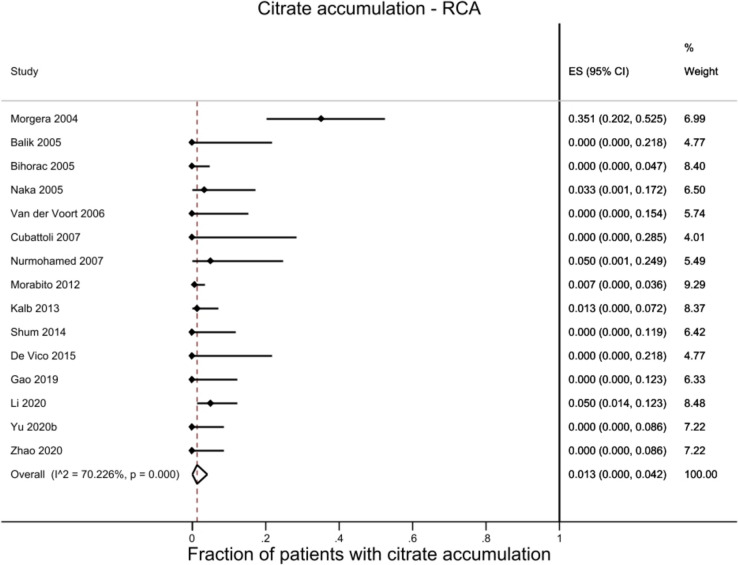
Results: Seventy-two studies were eligible for this meta-analysis. Statistically significant differences between heparin and RCA were observed in ionized calcium levels (mmol/l; heparin 1.19, RCA 1.13), bleeding events (heparin 12.6%, RCA 2.4%), filter lifespan (hours; heparin 16.43, RCA 36.69), clotting issues (heparin 50.7%, RCA 21.3%), filter failure rate (heparin 67.7%, RCA 13.5%), hypocalcemia (heparin 0.1%, RCA 4.4%) and alkalosis (heparin 0.4%, RCA 6.6%) rates. Limitations include heterogeneity across studies, particularly for RCA, and potential biases, although the overall methodological quality ranged from moderate to low.
Conclusions: Based on the evidence presented, despite higher rates of hypocalcemia and alkalosis, RCA demonstrates advantages over heparin, including a reduction in bleeding events, prevention of filter clotting and improvement in filter lifespan. Additionally, the cost outcome demonstrated comparable statistics depending on the RCA protocol considered, which supports the potential cost-effectiveness of RCA. RCA provides clear clinical and potential organizational benefits and comparable cost statistics with a reasonable level of confidence in the evidence for the economic data.
Keywords: Anticoagulation; Clinical parameters; Costs; Economic evaluation; Meta-analyses; Regional citrate; Systematic literature review; Systemic heparin.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Conflict of Interest: Carla Rognoni and Rosanna Tarricone (CERGAS, SDA Bocconi School of Management) have nothing to disclose. Robert Pohlmeier is an employee of Fresenius Medical Care Deutschland GmbH. Ethical Approval: This article is based on previously conducted studies and does not contain any new studies with human participants or animals performed by any of the authors.
Figures











References
-
- Kellum JA, Romagnani P, Ashuntantang G, Ronco C, Zarbock A, Anders H-J. Acute kidney injury. Nat Rev Dis Primer. 2021;7:1–17. - PubMed
-
- Zarbock A, Küllmar M, Kindgen-Milles D, Wempe C, Gerss J, Brandenburger T, et al. Effect of regional citrate anticoagulation vs systemic heparin anticoagulation during continuous kidney replacement therapy on dialysis filter life span and mortality among critically ill patients with acute kidney injury. JAMA. 2020;324:1–11. - PMC - PubMed
-
- Janssen MJFM, van der Meulen J. The bleeding risk in chronic haemodialysis: preventive strategies in high-risk patients. Neth J Med. 1996;48:198–207. - PubMed
-
- Acute Kidney Injury (AKI)—KDIGO. [cited 2023 Nov 20]. https://kdigo.org/guidelines/acute-kidney-injury/.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
