

Evidence-based Emergency Tracheal Intubation
- PMID: 40238943
- PMCID: PMC12264701
- DOI: 10.1164/rccm.202411-2165CI
Evidence-based Emergency Tracheal Intubation
Abstract
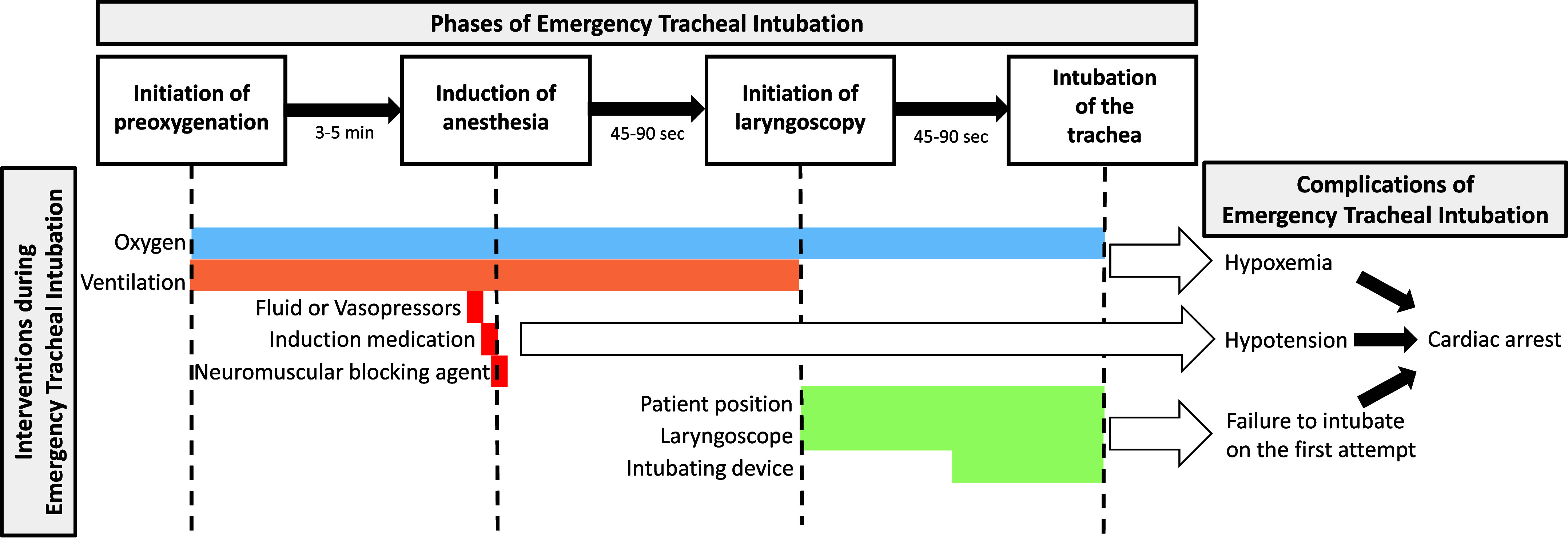
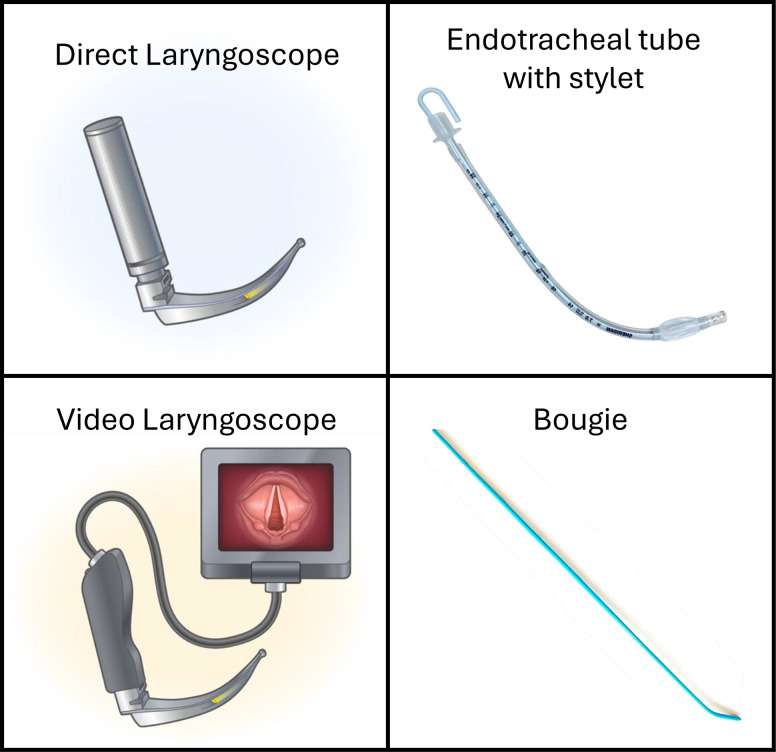
Millions of critically ill adults undergo tracheal intubation in an emergency department or ICU each year, nearly 40% of whom experience hypoxemia, hypotension, or cardiac arrest during the procedure. Over the last two decades, a series of randomized trials have examined which of the tools, techniques, devices, and drugs used to perform emergency tracheal intubation improve outcomes and which are ineffective or harmful. Results of these trials have demonstrated that preoxygenation with noninvasive ventilation and administration of positive pressure ventilation between induction and laryngoscopy prevent hypoxemia during intubation, video laryngoscopy facilitates successful intubation on the first attempt and may prevent esophageal intubation, use of a stylet is superior to intubation with an endotracheal tube alone and is comparable with use of a bougie, and administration of a fluid bolus before induction does not prevent hypotension. Many additional decisions clinicians face during emergency tracheal intubation are not yet informed by rigorous evidence. Randomized trials must continue to examine systematically each aspect of this common and high-risk procedure to improve patient outcomes and bring forth an era of evidence-based emergency tracheal intubation.
Keywords: emergency tracheal intubation; induction medication; laryngoscopy; preoxygenation.
Figures
References
-
- Pfuntner A, Wier L, Stocks C. Rockville, MD: Agency for Healthcare Research and Quality; 2013. Most frequent procedures performed in US hospitals, 2010.https://www.hcup-us.ahrq.gov/reports/statbriefs/sb149.jsp Statistical Brief #149. - PubMed
-
- Mosier JM, Sakles JC, Law JA, Brown CA, Brindley PG. Tracheal intubation in the critically ill. Where we came from and where we should go. Am J Respir Crit Care Med . 2020;201:775–788. - PubMed
-
- Acquisto NM, Mosier JM, Bittner EA, Patanwala AE, Hirsch KG, Hargwood P. et al. Society of Critical Care Medicine clinical practice guidelines for rapid sequence intubation in the critically ill adult patient. Crit Care Med . 2023;51:1411–1430. - PubMed
-
- Apfelbaum JL, Hagberg CA, Connis RT, Abdelmalak BB, Agarkar M, Dutton RP. et al. 2022 American Society of Anesthesiologists practice guidelines for management of the difficult airway. Anesthesiology . 2022;136:31–81. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
