

Sex Differences in Outcomes After Tenecteplase for Minor Stroke: A Subanalysis of the TEMPO-2 Trial
- PMID: 40240937
- PMCID: PMC12184240
- DOI: 10.1161/JAHA.124.039154
Sex Differences in Outcomes After Tenecteplase for Minor Stroke: A Subanalysis of the TEMPO-2 Trial
Abstract
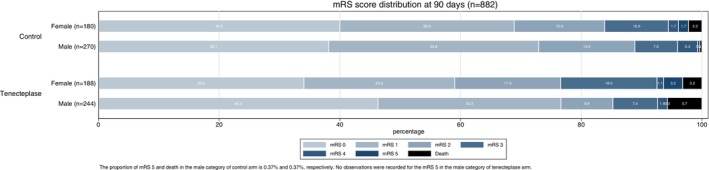
Background: In this subanalysis of the TEMPO-2 (Tenecteplase Versus Standard of Care for Minor Ischaemic Stroke With Proven Occlusion) trial, a randomized clinical trial comparing tenecteplase and nonthrombolytic control in patients with minor stroke and symptomatic intracranial occlusion, we investigated sex differences in the efficacy and safety of tenecteplase.
Methods: We compared outcomes after tenecteplase versus control, stratified by sex. We also compared outcomes in female versus male patients treated with tenecteplase. The primary outcome was a "responder" outcome, defined as return to baseline modified Rankin Scale score at 90 days. Secondary outcomes included the Lawton Instrumental Activities of Daily Living Scale, the EuroQol-5 Dimension, vessel recanalization, and adverse events. We used generalized linear modeling with a Poisson distribution adjusted for baseline differences to calculate adjusted risk ratios (aRR) and 95% CIs.
Results: There were 884 patients in the intention-to-treat analysis (48.9% tenecteplase, 41.5% female). Among female participants, the tenecteplase group was less likely to be a responder compared with control (63.8% tenecteplase, 73.9% control, aRR, 0.87 [95% CI, 0.76-1.00]). Among male participants, the responder outcome was similar between groups (77.5% tenecteplase, 75.4% control, 1.03 [95% CI, 0.94-1.13]). Female participants randomized to tenecteplase were less likely to be responders than male counterparts (63.8% female, 77.5% male, 0.85 [95% CI, 0.75-0.96]). Early recanalization was more frequent after tenecteplase than control in both sexes.
Conclusions: Tenecteplase was not associated with better clinical outcomes over nonthrombolytic control in female or male patients with minor ischemic stroke, despite more frequent recanalization. Fewer women treated with tenecteplase returned to baseline function compared with men.
Keywords: minor ischemic stroke; sex; stroke; thrombolysis.
Conflict of interest statement
Amy Y. X. Yu holds a Tier 2 Canada Research Chair in Data‐driven design of stroke systems and has received operating grant funding from the Heart and Stroke Foundation of Canada and the Canadian Institutes of Health Research. Aravind Ganesh reports a grant from Microvention and speaker fees from Alexion, Biogen and Servier Canada. Aravind Ganesh holds stock options for SnapDx Inc and Collavidence Inc. Thalia S. Field reports advisory board participation for AstraZeneca, Bayer, HLS Therapeutics, and Novartis and speaker's bureau for AstraZeneca. She is on the boards of Destine Health and the Vancouver General hospital/UBC Hospital Foundation and has served as an expert witness. Keith W. Muir reports funding from the British Heart Foundation (CS/18/5/34081) for this study. Michael D. Hill reports grant funding from Canadian Institutes of Health Research, Heart and Stroke Foundation of Canada, Alberta Innovates, and study drug from Boehringer‐Ingelheim. He also reports grants from NoNo and Medtronic. He has had consulting fees from Sun Pharma Brainsgate Inc. Shelagh B. Coutts reports grant funding from Canadian Institutes of Health Research, Heart and Stroke Foundation of Canada, and the British Heart Foundation to complete the TEMPO‐2 study. Boehringer Ingelheim provides the study drug (tenecteplase) for the study.
Figures

Comment in
-
Tenecteplase for Minor Stroke: Does Sex Matter?J Am Heart Assoc. 2025 May 6;14(9):e041733. doi: 10.1161/JAHA.125.041733. Epub 2025 Apr 16. J Am Heart Assoc. 2025. PMID: 40240931 Free PMC article. No abstract available.
References
-
- Coutts SB, Ankolekar S, Appireddy R, Arenillas JF, Assis Z, Bailey P, Barber PA, Bazan R, Buck BH, Butcher KS, et al. Tenecteplase versus standard of care for minor ischaemic stroke with proven occlusion (TEMPO‐2): a randomised, open label, phase 3 superiority trial. Lancet. 2024;403:2597–2605. doi: 10.1016/s0140-6736(24)00921-8 - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
