

Heavy Strength Training in Older Adults: Implications for Health, Disease and Physical Performance
- PMID: 40241440
- PMCID: PMC12003923
- DOI: 10.1002/jcsm.13804
Heavy Strength Training in Older Adults: Implications for Health, Disease and Physical Performance
Erratum in
-
Correction to 'Heavy Strength Training in Older Adults: Implications for Health, Disease and Physical Performance'.J Cachexia Sarcopenia Muscle. 2025 Aug;16(4):e70014. doi: 10.1002/jcsm.70014. J Cachexia Sarcopenia Muscle. 2025. PMID: 40717445 Free PMC article. No abstract available.
Abstract
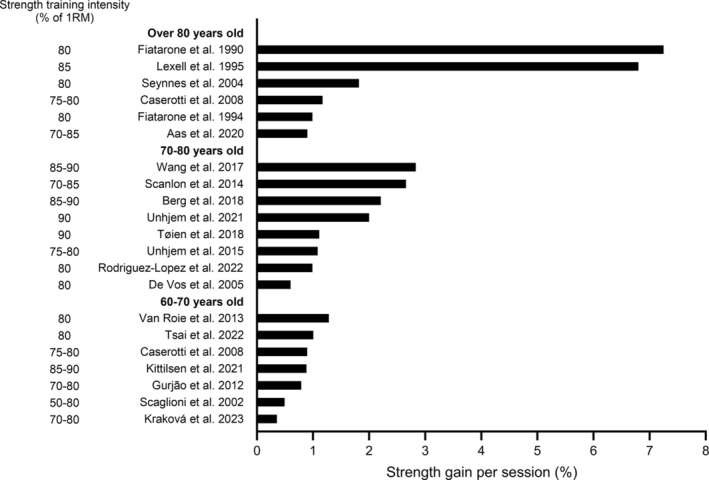
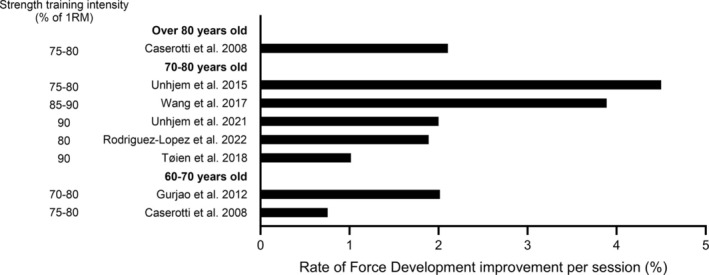
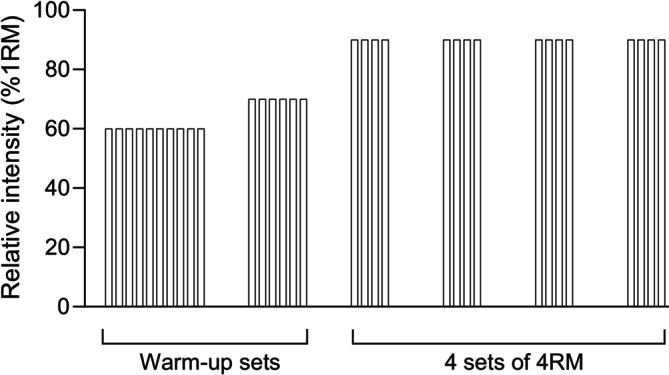
Older adults typically exhibit reductions in skeletal muscle maximal strength and the ability to produce force rapidly. These reductions are often augmented by concomitant acute and chronic diseases, resulting in attenuated physical performance and higher propensity of falls and injuries. With the proportion of older adults in the population increasing, there is an alarming need for cost-effective strategies to improve physical performance and combat a multitude of age-related diseases. Surprisingly, despite convincing evidence emerging over three decades that strength training can substantially improve maximal strength (1RM), rate of force development (RFD) and power, contributing to improved health, physical performance and fall prevention, it appears that it has not fully arrived at the older adults' doorsteps. The aim of the current narrative review is to accentuate the convincing benefits of strength training in healthy and diseased older adults. As intensity appears to play a key role for improvements in 1RM, RFD and power, this review will emphasize training performed with heavy (80%-84% of 1RM) and very heavy loads (≥ 85% of 1RM), where the latter is often referred to as maximal strength training (MST). MST uses loads of ~90% of 1RM, which can only be performed a maximum of 3-5 times, 3-5 sets and maximal intentional concentric velocity. Strength training performed with loads in the heavy to very heavy domain of the spectrum may, because of the large increases in muscle strength, focuses on neural adaptations and relatively low risk, provides additional benefits for older adults and contrasts current guidelines which recommend low-to-moderate intensity (60%-70% of 1RM) and slow-moderate concentric velocity. This review also provides information on practical application of MST aimed at practitioners who are involved with preventive and/or rehabilitative health care for older adults.
Keywords: heavy resistance training; high load; intended velocity; maximal strength training; rehabilitation.
© 2025 The Author(s). Journal of Cachexia, Sarcopenia and Muscle published by Wiley Periodicals LLC.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures

Similar articles
-
Dose-Response Relationships of Resistance Training in Healthy Old Adults: A Systematic Review and Meta-Analysis.Sports Med. 2015 Dec;45(12):1693-720. doi: 10.1007/s40279-015-0385-9. Sports Med. 2015. PMID: 26420238 Free PMC article.
-
Falls prevention interventions for community-dwelling older adults: systematic review and meta-analysis of benefits, harms, and patient values and preferences.Syst Rev. 2024 Nov 26;13(1):289. doi: 10.1186/s13643-024-02681-3. Syst Rev. 2024. PMID: 39593159 Free PMC article.
-
The importance of trunk muscle strength for balance, functional performance, and fall prevention in seniors: a systematic review.Sports Med. 2013 Jul;43(7):627-41. doi: 10.1007/s40279-013-0041-1. Sports Med. 2013. PMID: 23568373
-
Physical exercise training interventions for children and young adults during and after treatment for childhood cancer.Cochrane Database Syst Rev. 2016 Mar 31;3(3):CD008796. doi: 10.1002/14651858.CD008796.pub3. Cochrane Database Syst Rev. 2016. PMID: 27030386 Free PMC article.
-
Sexual Harassment and Prevention Training.2024 Mar 29. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan–. 2024 Mar 29. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan–. PMID: 36508513 Free Books & Documents.
Cited by
-
Correction to 'Heavy Strength Training in Older Adults: Implications for Health, Disease and Physical Performance'.J Cachexia Sarcopenia Muscle. 2025 Aug;16(4):e70014. doi: 10.1002/jcsm.70014. J Cachexia Sarcopenia Muscle. 2025. PMID: 40717445 Free PMC article. No abstract available.
-
Nicotinamide and Pyridoxine in Muscle Aging: Nutritional Regulation of Redox, Inflammation, and Regeneration.Antioxidants (Basel). 2025 Jul 25;14(8):911. doi: 10.3390/antiox14080911. Antioxidants (Basel). 2025. PMID: 40867810 Free PMC article. Review.
References
-
- Manton K. G., Corder L. S., and Stallard E., “Estimates of Change in Chronic Disability and Institutional Incidence and Prevalence Rates in the U.S. Elderly Population From the 1982, 1984, and 1989 National Long Term Care Survey,” Journal of Gerontology 48 (1993): S153–S166. - PubMed
-
- Suetta C., Magnusson S. P., Beyer N., and Kjaer M., “Effect of Strength Training on Muscle Function in Elderly Hospitalized Patients,” Scandinavian Journal of Medicine & Science in Sports 17 (2007): 464–472. - PubMed
-
- Hoff J., Tjonna A. E., Steinshamn S., Hoydal M., Richardson R. S., and Helgerud J., “Maximal Strength Training of the Legs in COPD: A Therapy for Mechanical Inefficiency,” Medicine and Science in Sports and Exercise 39 (2007): 220–226. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Research Materials
