

Risk factors and outcomes of pediatric non-invasive respiratory support failure in Latin America
- PMID: 40241834
- PMCID: PMC11997567
- DOI: 10.1016/j.jointm.2024.09.001
Risk factors and outcomes of pediatric non-invasive respiratory support failure in Latin America
Abstract
Background: Noninvasive respiratory support (NRS) is standard in pediatric intensive care units (PICUs) for respiratory diseases, but its failure can lead to complications requiring invasive mechanical ventilation (IMV). This study aimed to identify risk factors for NRS failure in children with acute respiratory failure (ARF) in PICUs, and compare complications and outcomes between IMV-only and NRS failure patients.
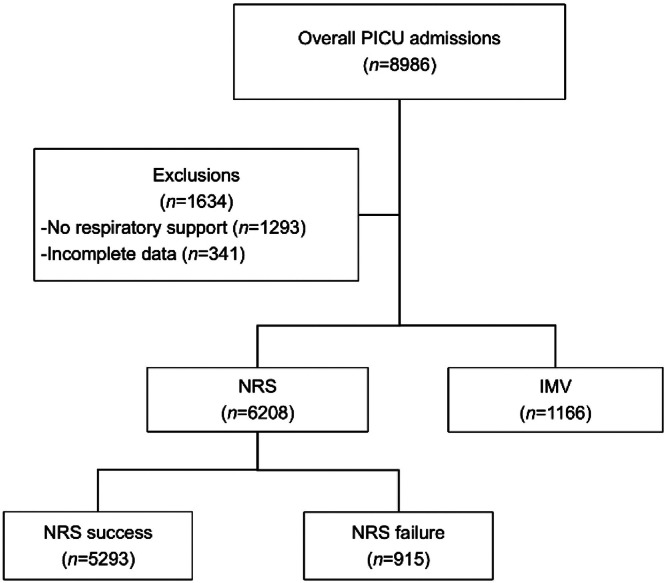
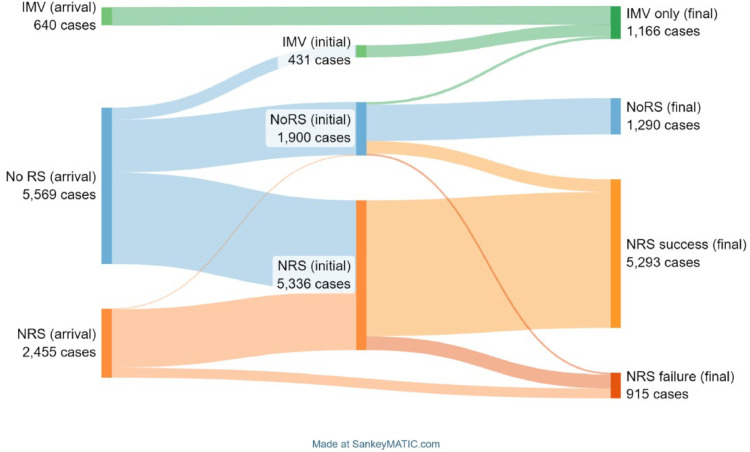
Methods: We conducted a cohort study using data from the LARed Network prospective registry (April 2017-November 2022), in children under 18 years admitted to PICUs for ARF. Cases were divided into subgroups: those managed with IMV only, those who experienced NRS failure requiring IMV, those who received NRS successfully, and those who did not require NRS or IMV. Exclusions included patients with home respiratory support prior to admission, patients without PICU discharge at the cutoff date of the analysis and those with incomplete data. Multivariate mixed models analyzed NRS failure risk factors, and complications between the IMV-only and NRS failure groups, using centers as a random effect.
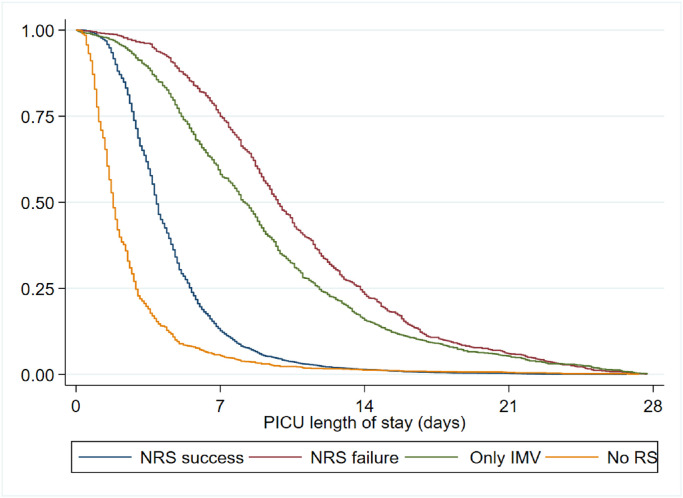
Results: A total of 7374 children met the inclusion criteria, with 6208 in the NRS group and 1166 in the IMV-only group. The NRS success rate was 85.3 %. Risk factors for NRS failure included age (median of 4.6 months, interquartile range of 2.1-14.2 months), history of prematurity (adjusted odds ratio [aOR]=1.53, 95 % confidence interval [CI]: 1.20 to 1.95) or malnutrition (aOR=1.85, 95 % CI: 1.18 to 2.91), suspected bacterial infection (aOR=5.12, 95 % CI: 4.05to 6.49), FiO2 >30 % (aOR=1.52, 95 % CI: 1.18 to 1.97), severe hypoxemia with SpO2/FiO2 ≤150 (aOR=1.85, 95 % CI: 1.48 to 2.30), tachypnea (aOR=1.42, 95 % CI: 1.18 to 1.72), tachycardia (aOR=1.77, 95 % CI: 1.47 to 2.12), and lung consolidations (aOR=1.45, 95 % CI: 1.14 to 1.85) or interstitial infiltrates (aOR=1.29, 95 % CI: 1.05 to 1.58) on chest X-ray. There were no significant differences in morbidity, mortality, duration of IMV, or PICU length of stay between patients who received IMV only and those who experienced NRS failure. However, patients who experienced NRS failure were more likely to develop withdrawal symptoms related to sedative or opioid discontinuation and/or delirium (aOR=2.57, 95 % CI: 1.85 to 2.57).
Conclusion: This study identified key risk factors for predicting NRS failure in children with acute ARF in PICUs, including younger age, prematurity, malnutrition, suspected bacterial infection, FiO2 >30 %, severe hypoxemia (SpO2/FiO2 ≤150), tachypnea, tachycardia, and radiological findings such as lung consolidation and interstitial infiltrates. Compared to patients managed with IMV from the start, those who experienced NRS failure were more likely to develop withdrawal symptoms and/or delirium, although clinical outcomes such as mortality, IMV duration, and PICU length of stay were similar in both groups.
Keywords: Continuous positive airway pressure; Noninvasive ventilation; Oxygen therapy; Pediatric intensive care unit; Pediatrics.
© 2024 The Author(s).
Figures
References
LinkOut - more resources
Full Text Sources
Miscellaneous
