

AutoCOPD-A novel and practical machine learning model for COPD detection using whole-lung inspiratory quantitative CT measurements: a retrospective, multicenter study
- PMID: 40242563
- PMCID: PMC12002883
- DOI: 10.1016/j.eclinm.2025.103166
AutoCOPD-A novel and practical machine learning model for COPD detection using whole-lung inspiratory quantitative CT measurements: a retrospective, multicenter study
Abstract
Background: The rate of diagnosis for chronic obstructive pulmonary disease (COPD) is low worldwide. Quantitative computed tomography (QCT) parameters add value to quantify alterations in airway and lung parenchyma for COPD. This study aimed to assess the performance of QCT features in COPD detection using a whole-lung inspiratory CT model.
Methods: This multicenter retrospective study was performed on 4106 participants. The derivation cohort containing 1950 participants who enrolled in Guangzhou communities from August 2017 to December 2019, was separated for training and internal validation cohorts, and three external validation cohorts containing 1703 participants were recruited from the public hospitals (Cohort 1: the First Affiliated Hospital of Guangzhou Medical University; Cohort 2: Xiangyang central hospital; Cohort 3: the Second Affiliated Hospital of Xi'an Jiaotong University) in China between April 2017 and May 2024. Questionnaire information, CT reports, and QCT features derived from inspiratory CT were extracted for model development. A novel multimodal framework using eXtreme gradient boosting and hybrid feature selection was established for COPD detection. National Lung Screening Trial (NLST) cohort (n = 453) was applied to validate the multiracial extrapolation and robustness on low-dose CT scans.
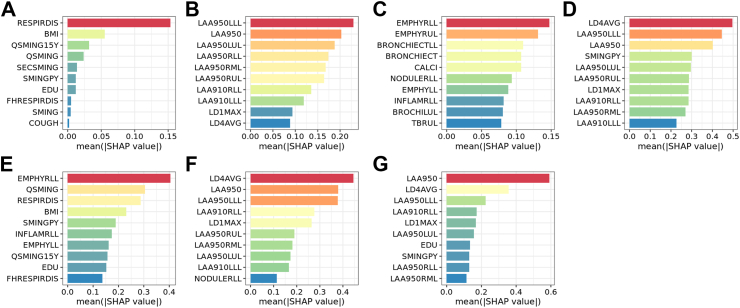
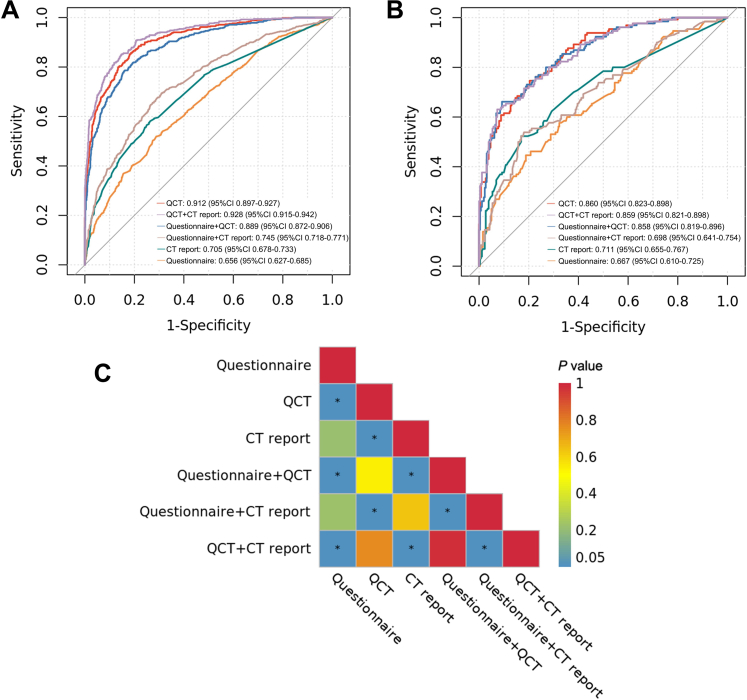
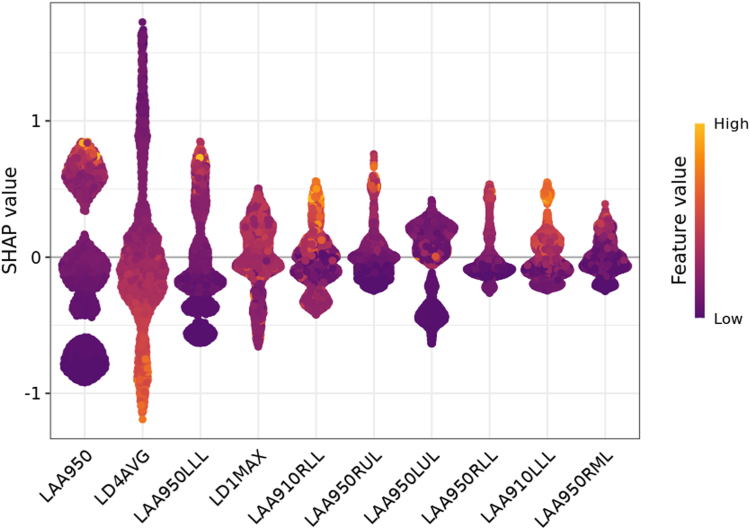
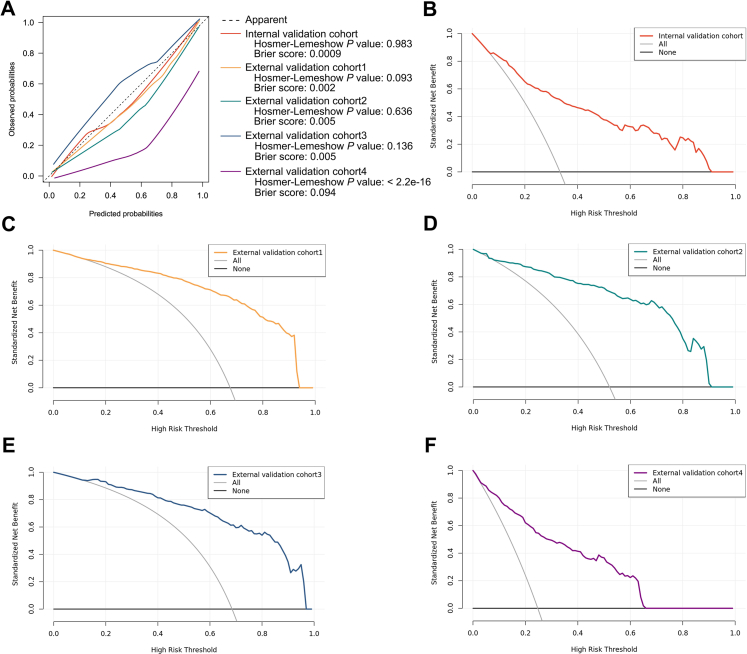
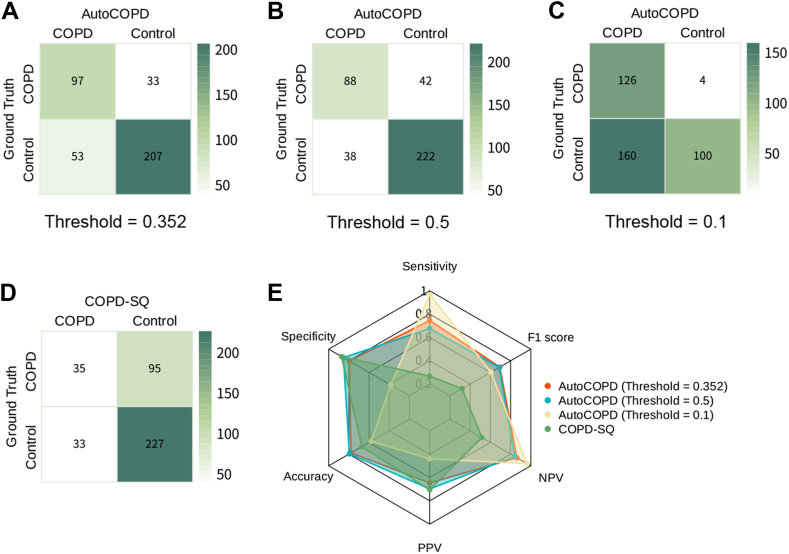
Findings: The QCT model (referred to as AutoCOPD) with ten features achieved the highest AUC of 0·860 (95% CI: 0·823-0·898) in the internal validation cohort, and showed excellent discrimination when externally validated [Cohort 1: AUC = 0·915 (95% CI: 0·898-0·931); Cohort 2: AUC = 0·903 (95% CI: 0·864-0·943); Cohort 3: AUC = 0·914 (95% CI: 0·882-0·947); NLST: AUC = 0·881 (95% CI: 0·846-0·915)]. Decision curve analysis demonstrated that AutoCOPD was valuable across a range of COPD risk thresholds between 0·12 and 0·66 compared with intervention in all patients with COPD or no intervention.
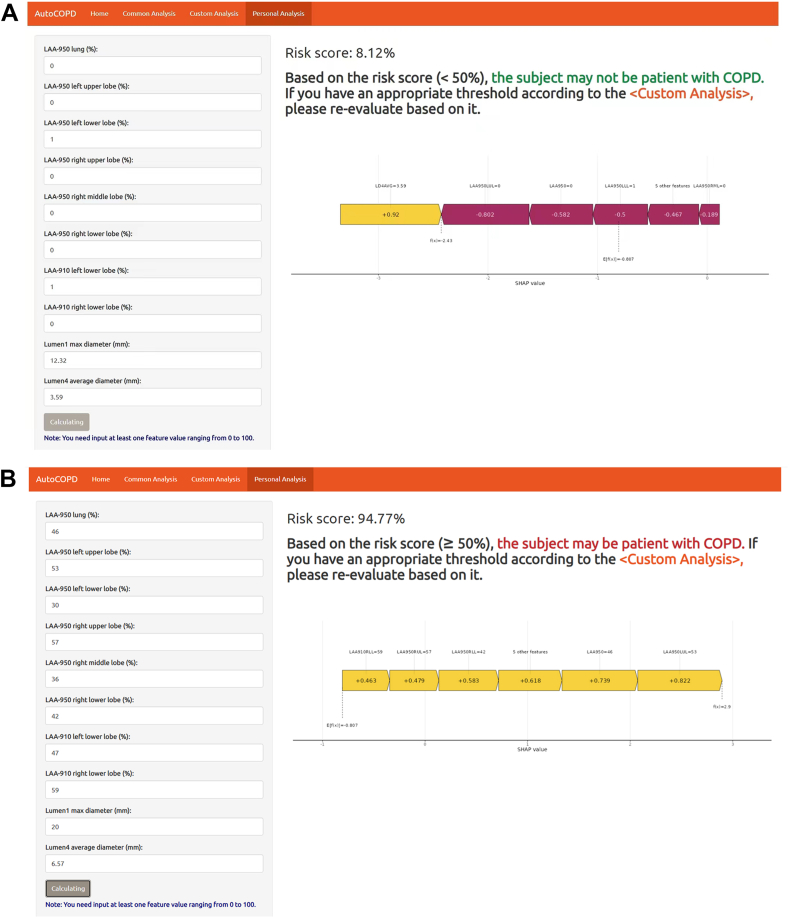
Interpretation: Heterogeneous COPD can be well identified using AutoCOPD (https://lwj-lab.shinyapps.io/autocopd/) constructed by a subset of only ten QCT features. It may be generalizable across clinical settings and serve as a feasible tool for early detecting patients with mild or asymptomatic COPD to reduce delayed diagnosis in routine practice.
Funding: The National Natural Science Foundation of China, Guangzhou Laboratory, Natural Science Foundation of Guangdong Province, Guangzhou Municipal Science and Technology grant, State Key Laboratory of Respiratory Disease.
Keywords: COPD; Detection; Machine learning; Quantitative computed tomography.
© 2025 The Authors.
Conflict of interest statement
CL is a senior engineer of Neusoft Medical Systems, a leading company of global information technology, product, and solution. WL received free access to the NeuLungCare–QA software for CT images analysis provided by Neusoft Medical Systems, and received free technical support from Guangzhou Tianpeng Computer Technology Co., Ltd. FL received free access to NCI's data collected by NLST. All other authors do not have any potential conflicts of interest to declare.
Figures
References
-
- Global initiative for chronic obstructive lung disease . GOLD Science Committee; 2024. Global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease (2025 REPORT)https://goldcopd.org/2025-gold-report/ [accessed 2024 Nov]. Available from:
-
- Wang C., Xu J., Yang L., et al. Prevalence and risk factors of chronic obstructive pulmonary disease in China (the China Pulmonary Health [CPH] study): a national cross-sectional study. Lancet. 2018;391:1706–1717. - PubMed
-
- Diab N., Gershon A.S., Sin D.D., et al. Underdiagnosis and overdiagnosis of chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2018;198:1130–1139. - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous
