

Effectiveness of Tolvaptan for Autosomal Dominant Polycystic Kidney Disease in US Clinical Practice With Comparison to Historical Control Data
- PMID: 40242785
- PMCID: PMC12002913
- DOI: 10.1016/j.xkme.2025.100988
Effectiveness of Tolvaptan for Autosomal Dominant Polycystic Kidney Disease in US Clinical Practice With Comparison to Historical Control Data
Abstract
Rationale & objective: Data from clinical practice are needed to characterize the effectiveness of pharmacotherapy outside the controlled setting of clinical trials but lack an untreated placebo group for comparison. To assess the effectiveness of tolvaptan for autosomal dominant polycystic kidney disease (ADPKD) in nephrology practice, we performed a chart review of US patients and compared it with a historical matched control cohort.
Study design: Patient data from charts were provided by US nephrologists who participated in an online survey. Historical control data for patients with ADPKD not treated with tolvaptan were extracted from a database of ADPKD clinical studies (Consortium for Radiologic Imaging Studies of Polycystic Kidney Disease, HALT Progression of Polycystic Kidney Disease, and OVERTURE).
Setting & participants: Nephrologist respondents (n = 57) provided baseline data and up to 4 years of follow-up on estimated glomerular filtration rate (eGFR) for tolvaptan-treated adults (n = 149). Historical ADPKD-affected controls were adults in Mayo imaging risk classes 1C-1E (ie, at increased risk of rapid progression, consistent with the tolvaptan indication).
Exposure: Cases had to receive tolvaptan continuously for ≥2 years. Historical controls received nontolvaptan standard of care, including various antihypertensive regimens.
Outcome: Annual rate of eGFR change.
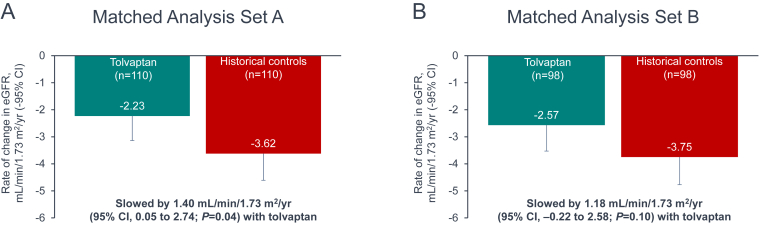
Analytical approach: Cases and controls were matched on baseline clinical characteristics (matched set A: age, sex, and chronic kidney disease stage [110 matched pairs]; matched set B: age, sex, and eGFR [98 matched pairs]) and compared using a mixed model.
Results: The annual rate of eGFR decline was slower in tolvaptan-treated patients versus historical controls, by 1.40 mL/min/1.73 m2 (95% CI, 0.05-2.74; P = 0.04) in set A. Set B demonstrated a similar trend: 1.18 mL/min/1.73 m2 per year (95% CI, -0.22 to 2.58; P = 0.10).
Limitations: Risk of bias from convenience sampling and potential residual confounding after case/historical control matching.
Conclusions: Tolvaptan was associated with slower eGFR decline in routine clinical practice, consistent with the results of controlled trials.
Keywords: Autosomal dominant polycystic kidney disease; clinical practice; estimated glomerular filtration rate; historical control study; tolvaptan.
Plain language summary
Randomized, controlled trials are the gold standard for evaluating pharmacotherapy, but evidence collected under routine clinical conditions can answer questions about drug effectiveness, safety, and value that are particularly relevant to everyday medical practice. Trial data have demonstrated that tolvaptan slows kidney function decline in patients with autosomal dominant polycystic kidney disease who are at increased risk of rapid progression. To assess treatment effect in regular nephrology practice, we invited US nephrologists to provide anonymized data on patients receiving tolvaptan under their care. We compared decline in estimated glomerular filtration rate in the tolvaptan-treated group with matched historical controls who did not receive tolvaptan. Across multiple matched analysis sets, tolvaptan slowed estimated glomerular filtration rate decline over a 4-year follow-up period.
© 2025 The Authors.
Figures


References
-
- Torres V.E., Chapman A.B., Devuyst O., et al. Multicenter, open-label, extension trial to evaluate the long-term efficacy and safety of early versus delayed treatment with tolvaptan in autosomal dominant polycystic kidney disease: the TEMPO 4:4 Trial. Nephrol Dial Transplant. 2018;33(3):477–489. doi: 10.1093/ndt/gfx043. - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
