

Wound morphologies of sclerotomies closed with scleral massage and scleral needling techniques: A comparative study
- PMID: 40243079
- PMCID: PMC12178354
- DOI: 10.4103/IJO.IJO_2184_24
Wound morphologies of sclerotomies closed with scleral massage and scleral needling techniques: A comparative study
Abstract
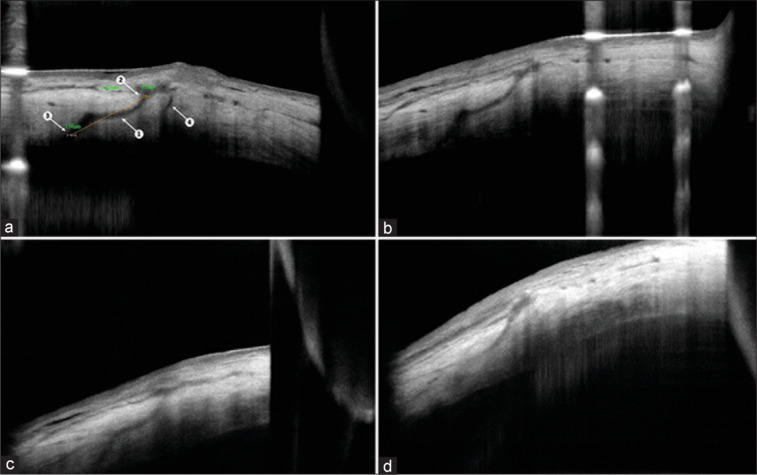
Background: This prospective study aimed to compare scleral needling with the conventional scleral massage technique for sclerotomy closure, using anterior segment optical coherence tomography (AS-OCT) to assess postoperative wound morphology.
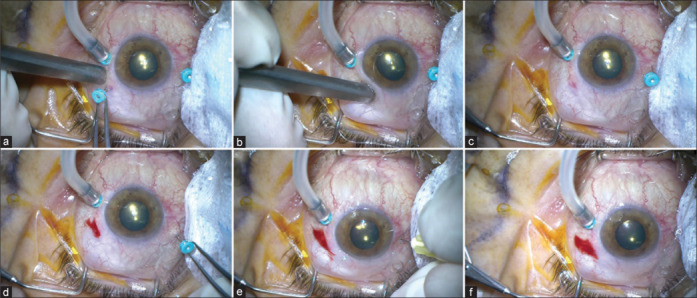
Methods: Thirty eyes of 30 patients undergoing pars plana vitrectomy with a 25G vitrectomy system (Constellation; Alcon Laboratories, Fort Worth, TX, USA) were included. In each eye, one superior sclerotomy site (superonasal or superotemporal) was closed with scleral needling (Group A), while the other was closed with scleral massage (Group B), eliminating the impact of individual variability.
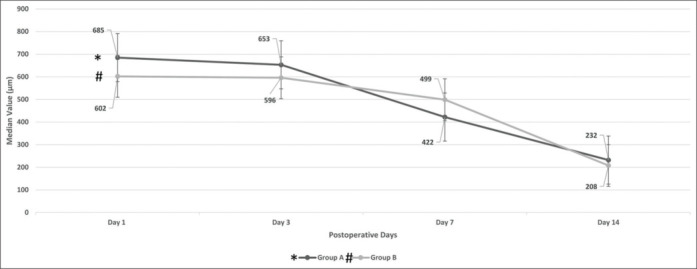
Results: Most sclerotomies (80%) could be closed with a single attempt of needling (mean 1.2 ± 0.4). The mean outer and inner sclerotomy incision diameters on the postoperative first day were 119 ± 22 and 94 ± 17 µm, respectively, for group A, and 118 ± 19 and 94 ± 16 µm, respectively, for group B ( P = 0.658 and 0.871, respectively). Sclerotomy wound diameters of both groups A and B decreased significantly on postoperative day 14 ( P < 0.001 and P < 0.001, respectively). None of the patients developed postoperative hypotony or any severe complication. A conjunctival bleb in four Group A patients resolved by day 3.
Conclusion: The newly described scleral needling technique was as successful and safe as the conventional scleral massage technique. AS-OCT imaging also confirmed that scleral needling did not cause any disruption on wound morphology.
Keywords: AS-OCT; scleral massage; scleral needling; sclerotomy incisions; sutureless vitrectomy.
Copyright © 2025 Indian Journal of Ophthalmology.
Conflict of interest statement
There are no conflicts of interest.
Figures
Similar articles
-
Modified Scleral Needling Technique to Achieve Scleral Wound Closure in Microincision Vitrectomy Surgery.Cureus. 2025 May 23;17(5):e84700. doi: 10.7759/cureus.84700. eCollection 2025 May. Cureus. 2025. PMID: 40556991 Free PMC article.
-
Evaluation of wound closure in oblique 23-gauge sutureless sclerotomies with visante optical coherence tomography.Am J Ophthalmol. 2009 Jan;147(1):101-107.e1. doi: 10.1016/j.ajo.2008.07.046. Epub 2008 Oct 4. Am J Ophthalmol. 2009. PMID: 18835474
-
Effect of intravitreal gas tamponade for sutureless vitrectomy wounds: three-dimensional corneal and anterior segment optical coherence tomography study.Retina. 2011 Apr;31(4):702-6. doi: 10.1097/IAE.0b013e3181f0d2e6. Retina. 2011. PMID: 21242862
-
Prenatal administration of progestogens for preventing spontaneous preterm birth in women with a multiple pregnancy.Cochrane Database Syst Rev. 2019 Nov 20;2019(11):CD012024. doi: 10.1002/14651858.CD012024.pub3. Cochrane Database Syst Rev. 2019. PMID: 31745984 Free PMC article.
-
Pharmacological and electronic cigarette interventions for smoking cessation in adults: component network meta-analyses.Cochrane Database Syst Rev. 2023 Sep 12;9(9):CD015226. doi: 10.1002/14651858.CD015226.pub2. Cochrane Database Syst Rev. 2023. PMID: 37696529 Free PMC article.
References
-
- Fujii GY, de Juan E, Jr, Humayun MS, Pieramici DJ, Chang TS, Awh C, et al. A new 25-gauge instrument system for transconjunctival sutureless vitrectomy surgery. Ophthalmology. 2002;109:1807–12. - PubMed
-
- Eckardt C. Transconjunctival sutureless 23-gauge vitrectomy. Retina. 2005;25:208–11. - PubMed
-
- Oshima Y, Wakabayashi T, Sato T, Ohji M, Tano Y. A 27–gauge instrument system for transconjunctival sutureless microincision vitrectomy surgery. Ophthalmology. 2010;117:93–102.e2. - PubMed
-
- Romano MR, Cennamo G, Ferrara M, Cennamo M, Cennamo G. Twenty-seven-gauge versus 25-gauge vitrectomy for primary rhegmatogenous retinal detachment. Retina. 2017;37:637–42. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
