

Prediction of Primary Admission Total Charges Following Single-Level Lumbar Arthrodesis Utilizing Machine Learning
- PMID: 40243119
- PMCID: PMC12006119
- DOI: 10.1177/21925682251336714
Prediction of Primary Admission Total Charges Following Single-Level Lumbar Arthrodesis Utilizing Machine Learning
Abstract
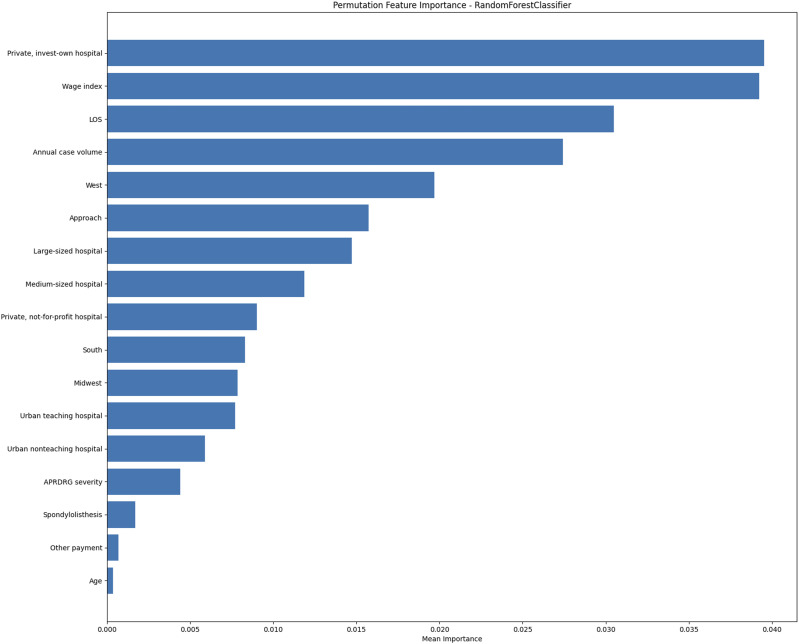
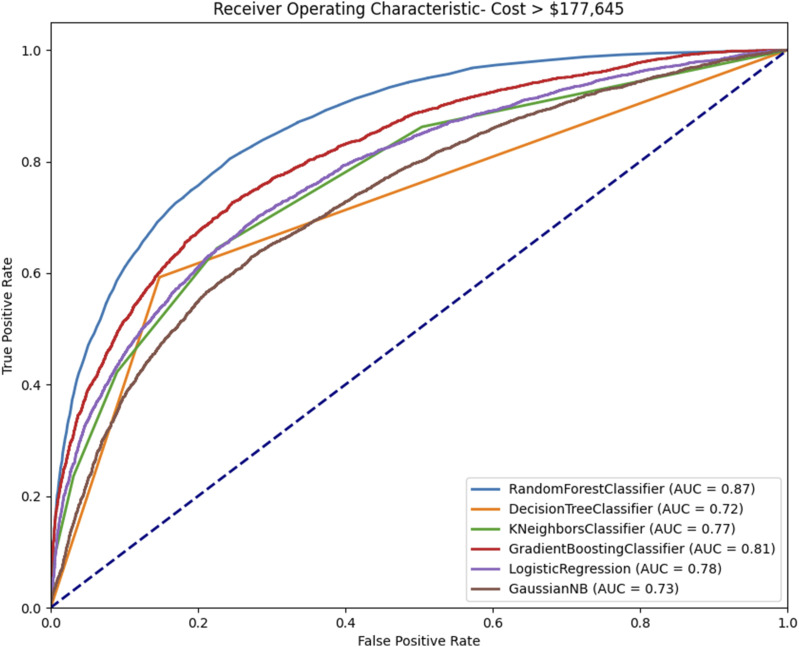
Study DesignRetrospective analysis utilizing machine learning.ObjectivesThis study aims to identify the key factors influencing total charges during the primary admission period following single-level lumbar arthrodesis, using machine learning models to enhance predictive accuracy.MethodsData were extracted from the National Inpatient Sample (NIS) database and analyzed using various machine learning models, including random forest, gradient boosting trees, and logistic regression. A total of 78,022 unweighted cases of patients who underwent single-level lumbar arthrodesis were identified using the NIS database from 2016 to 2020. Variables included hospital size, region, patient-specific factors, and procedural details. Multivariate linear regression was also used to identify charge-related variables.ResultsThe average total charge for single-level lumbar arthrodesis was $145,600 ± $102,500. Significant predictors of charge included length of stay, hospital size, hospital ownership, and region. Private investor-owned hospitals and procedures performed in the Western U.S. were associated with higher charges. Random forest models demonstrated superior predictive accuracy with an AUC of .866, outperforming other models.ConclusionsHospital characteristics, regional factors, and patient-specific variables significantly influence the charges of single-level lumbar arthrodesis. Machine learning models, particularly random forest, provide robust tools for predicting healthcare costs, enabling better resource allocation and decision-making. Future research should explore these dynamics further to optimize cost management and improve care quality.
Keywords: cost-effectiveness; lumbar arthrodesis; lumbar fusion; machine learning; national inpatient sample; value-based care.
Conflict of interest statement
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Mitchell K. Ng is a paid consultant at Pacira BioSciences Inc., Sage Products Inc., Alafair Biosciences Inc., Next Science LLC, Bonutti Technologies Inc., Johnson & Johnson Ethicon Inc., Hippocrates Opportunities Fund LLC, and Ferghana Partners Inc.
Figures
Similar articles
-
Prediction of primary admission total charges following cervical disc arthroplasty utilizing machine learning.Spine J. 2025 Mar;25(3):429-438. doi: 10.1016/j.spinee.2024.09.025. Epub 2024 Sep 26. Spine J. 2025. PMID: 39332690
-
Machine learning ensemble models predict total charges and drivers of cost for transsphenoidal surgery for pituitary tumor.J Neurosurg. 2018 Sep 21;131(2):507-516. doi: 10.3171/2018.4.JNS18306. Print 2019 Aug 1. J Neurosurg. 2018. PMID: 30239321
-
Predicting postoperative outcomes in lumbar spinal fusion: development of a machine learning model.Spine J. 2024 Feb;24(2):239-249. doi: 10.1016/j.spinee.2023.09.029. Epub 2023 Oct 20. Spine J. 2024. PMID: 37866485
-
Can Predictive Modeling Tools Identify Patients at High Risk of Prolonged Opioid Use After ACL Reconstruction?Clin Orthop Relat Res. 2020 Jul;478(7):0-1618. doi: 10.1097/CORR.0000000000001251. Clin Orthop Relat Res. 2020. PMID: 32282466 Free PMC article.
-
Supervised Machine Learning for Predicting Length of Stay After Lumbar Arthrodesis: A Comprehensive Artificial Intelligence Approach.J Am Acad Orthop Surg. 2022 Feb 1;30(3):125-132. doi: 10.5435/JAAOS-D-21-00241. J Am Acad Orthop Surg. 2022. PMID: 34928886
References
-
- Russo AJ, Schopler SA, Stetzner KJ, Shirk T. Minimally invasive transforaminal lumbar interbody fusion with expandable articulating interbody spacers significantly improves radiographic outcomes compared to static interbody spacers. J Spine Surg. 2021;7(3):300-309. doi:10.21037/JSS-20-630 - DOI - PMC - PubMed
-
- Doria C, Lisai P, Meloni GB, Pala PP, Serra M, Fabbriciani C. Instrumented posterior interbody fusion in degenerative and multioperated lumbar spine. J Orthop Traumatol. 2004;5(1):20-25. doi:10.1007/S10195-004-0035-8/METRICS - DOI
LinkOut - more resources
Full Text Sources
