

Derivation and validation of an artificial intelligence-based plaque burden safety cut-off for long-term acute coronary syndrome from coronary computed tomography angiography
- PMID: 40243706
- PMCID: PMC12206583
- DOI: 10.1093/ehjci/jeaf121
Derivation and validation of an artificial intelligence-based plaque burden safety cut-off for long-term acute coronary syndrome from coronary computed tomography angiography
Abstract
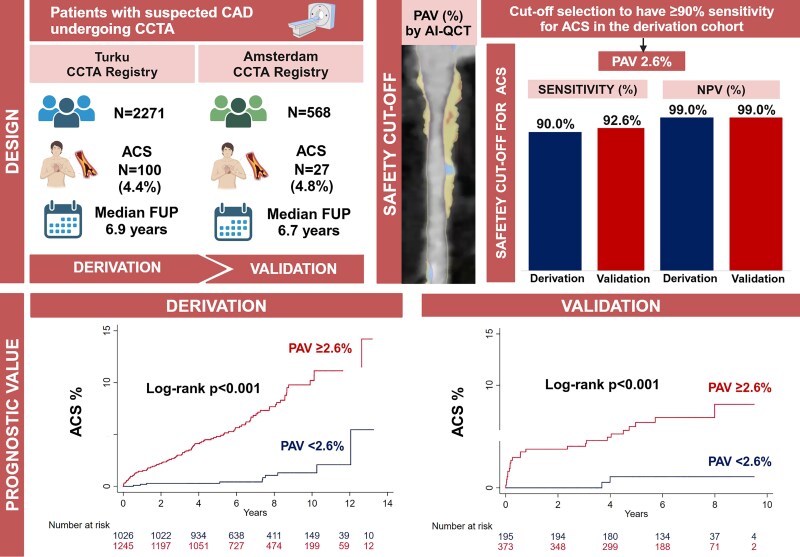
Aims: Artificial intelligence (AI) has enabled accurate and fast plaque quantification from coronary computed tomography angiography (CCTA). However, AI detects any coronary plaque in up to 97% of patients. To avoid overdiagnosis, a plaque burden safety cut-off for future coronary events is needed.
Methods and results: Percent atheroma volume (PAV) was quantified with AI-guided quantitative computed tomography in a blinded fashion. Safety cut-off derivation was performed in the Turku CCTA registry (Finland), and pre-defined as ≥90% sensitivity for acute coronary syndrome (ACS). External validation was performed in the Amsterdam CCTA registry (the Netherlands). In the derivation cohort, 100/2271 (4.4%) patients experienced ACS (median follow-up 6.9 years). A threshold of PAV ≥ 2.6% was derived with 90.0% sensitivity and negative predictive value (NPV) of 99.0%. In the validation cohort 27/568 (4.8%) experienced ACS (median follow-up 6.7 years) with PAV ≥ 2.6% showing 92.6% sensitivity and 99.0% NPV for ACS. In the derivation cohort, 45.2% of patients had PAV < 2.6 vs. 4.3% with PAV 0% (no plaque) (P < 0.001) (validation cohort: 34.3% PAV < 2.6 vs. 2.6% PAV 0%; P < 0.001). Patients with PAV ≥ 2.6% had higher adjusted ACS rates in the derivation [Hazard ratio (HR) 4.65, 95% confidence interval (CI) 2.33-9.28, P < 0.001] and validation cohort (HR 7.31, 95% CI 1.62-33.08, P = 0.010), respectively.
Conclusion: This study suggests that PAV up to 2.6% quantified by AI is associated with low-ACS risk in two independent patient cohorts. This cut-off may be helpful for clinical application of AI-guided CCTA analysis, which detects any plaque in up to 96-97% of patients.
Keywords: acute coronary syndrome; artificial intelligence; coronary computed tomography angiography; plaque burden.
© The Author(s) 2025. Published by Oxford University Press on behalf of the European Society of Cardiology.
Conflict of interest statement
Conflict of interest: S.B. received research grants to the institution from Medis Medical Imaging Systems, Bangerter-Rhyner Stiftung (Basel, Switzerland), and Abbott outside the submitted work, speaker fees from Cleerly Inc. and travel fees from Sanofi. J.K. received consultancy fees from GE Healthcare and Synektik and speaker fees from Bayer, Lundbeck, Boehringer Ingelheim, Pfizer, and Siemens, outside of the submitted work. A.S. received consultancy fees from Astra Zeneca and Pfizer, and speaker fees from Abbott, Astra Zeneca, Janssen, Novartis, and Pfizer. J.J.B. received speaker fees from Abbott. N.S.N. reports grants from the Dutch Heart Foundation (Dekker 03-007-2023-0068), European Atherosclerosis Society (2023), research funding/speaker fees from Cleerly, Daiichi Sankyo and Novartis, and is co-founder of Lipid Tools. I.D. is a member of Cleerly Scientific Advisory Board and Associate Editor of the European Heart Journal Cardiovascular Imaging. P.K. has received research grants from Cleerly, Inc. and HeartFlow. All other authors have reported that they have no relationships relevant to the contents of this paper to disclose.
Figures


Comment in
-
When coronary plaque is found in everyone: is anyone really at risk?Eur Heart J Cardiovasc Imaging. 2025 Jun 30;26(7):1174-1175. doi: 10.1093/ehjci/jeaf137. Eur Heart J Cardiovasc Imaging. 2025. PMID: 40315302 No abstract available.
Similar articles
-
AI-Guided Quantitative Plaque Staging Predicts Long-Term Cardiovascular Outcomes in Patients at Risk for Atherosclerotic CVD.JACC Cardiovasc Imaging. 2024 Mar;17(3):269-280. doi: 10.1016/j.jcmg.2023.05.020. Epub 2023 Jul 19. JACC Cardiovasc Imaging. 2024. PMID: 37480907
-
CTA-Derived Plaque Characteristics and Risk of Acute Coronary Syndrome in Patients With Coronary Artery Calcium Score of Zero: Insights From the ICONIC Trial.AJR Am J Roentgenol. 2025 Jul;225(1):e2431476. doi: 10.2214/AJR.24.31476. Epub 2025 Apr 30. AJR Am J Roentgenol. 2025. PMID: 40304673
-
Interaction of AI-Enabled Quantitative Coronary Plaque Volumes on Coronary CT Angiography, FFRCT, and Clinical Outcomes: A Retrospective Analysis of the ADVANCE Registry.Circ Cardiovasc Imaging. 2024 Mar;17(3):e016143. doi: 10.1161/CIRCIMAGING.123.016143. Epub 2024 Mar 12. Circ Cardiovasc Imaging. 2024. PMID: 38469689
-
Systematic review of the clinical effectiveness and cost-effectiveness of 64-slice or higher computed tomography angiography as an alternative to invasive coronary angiography in the investigation of coronary artery disease.Health Technol Assess. 2008 May;12(17):iii-iv, ix-143. doi: 10.3310/hta12170. Health Technol Assess. 2008. PMID: 18462576
-
Plaque quantification from coronary computed tomography angiography in predicting cardiovascular events: A systematic review and meta-analysis.J Cardiovasc Comput Tomogr. 2025 Jul-Aug;19(4):423-432. doi: 10.1016/j.jcct.2025.05.003. Epub 2025 May 26. J Cardiovasc Comput Tomogr. 2025. PMID: 40425410
References
-
- Vrints C, Andreotti F, Koskinas KC, Rossello X, Adamo M, Ainslie J et al. 2024 ESC Guidelines for the management of chronic coronary syndromes: developed by the task force for the management of chronic coronary syndromes of the European Society of Cardiology (ESC) Endorsed by the European Association for Cardio-Thoracic Surgery (EACTS). Eur Heart J 2024;45:3415–537.
-
- Gulati M, Levy PD, Mukherjee D, Amsterdam E, Bhatt DL, Birtcher KK et al. 2021 AHA/ACC/ASE/CHEST/SAEM/SCCT/SCMR guideline for the evaluation and diagnosis of chest pain: a report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation 2021;16:54–122. - PubMed
-
- Griffin WF, Choi AD, Riess JS, Marques H, Chang HJ, Choi JH et al. AI evaluation of stenosis on coronary CTA, comparison with quantitative coronary angiography and fractional flow reserve. JACC Cardiovasc Imaging 2023;16:193–205. - PubMed
-
- Choi AD, Marques H, Kumar V, Griffin WF, Rahban H, Karlsberg RP et al. CT evaluation by artificial intelligence for atherosclerosis, stenosis and vascular morphology (CLARIFY): a multi-center, international study. J Cardiovasc Comput Tomogr 2021;15:470–6. - PubMed
