

Oversized Conduits Predict Stenosis in Tissue Engineered Vascular Grafts
- PMID: 40243957
- PMCID: PMC12434202
- DOI: 10.1016/j.jacbts.2025.02.008
Oversized Conduits Predict Stenosis in Tissue Engineered Vascular Grafts
Abstract
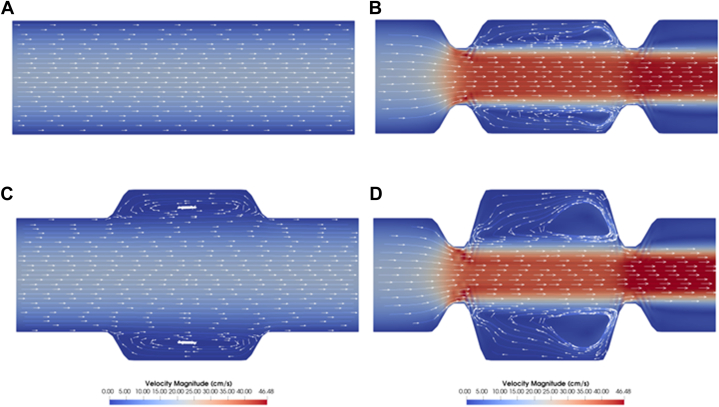
Tissue-engineered vascular grafts (TEVGs) offer promising advancements in treating congenital heart disease by enabling the creation of autologous tissue for complex cardiac repairs. Our approach involves implanting biodegradable scaffolds seeded with autologous cells that remodel into functional neovessels. To understand better the factors guiding neovessel formation, we evaluated 50 ovine thoracic TEVGs using angiography at 1 and 6 weeks postimplantation. Nondimensionalization accounted for anatomical differences between animals and identified hemodynamics and surgical sizing as potential driving factors. Regression analysis revealed that narrowing at the inflow anastomosis and graft oversizing correlated significantly with stenosis development. Computational fluid dynamics showed that these factors influenced wall shear stress and flow patterns, contributing to neovessel narrowing. Comparisons with clinical trial data from Fontan conduits supported these findings, emphasizing that matching graft size to the native inflow vessel can reduce stenosis and enhance TEVG performance.
Keywords: computational fluid dynamics; oversizing; stenosis; tissue engineered vascular graft.
Copyright © 2025 The Authors. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Funding Support and Author Disclosures This project was supported by National Institutes of Health grants R01 HL139796 (to Drs Humphrey, Marsden, and Breuer), R01 HL163065 (to Dr Breuer), and UH3 HL148693 (to Dr Breuer) in addition to Department of Defense award number W81XWH-22-1-0597 (to Dr Breuer). Dr Breuer is an inventor on patent/patent applications (2015252805 [Australia], 2016565483 [Japan], 855,370, 9,446,175, 9,782,522, 10,300,082, 61/987,910, 62/266,309, 62/309,285, 62/209,990, 62/936,225) submitted by Yale University and/or Nationwide Children’s Hospital that cover methods of improving the design, manufacturing, or performance of tissue-engineered vascular grafts; is a founder of Lyst Therapeutics; and has received grant support from Gunze Ltd, and Gunze Ltd provided support for the clinical trial. All other authors have reported that they have no relationships relevant to the contents of this paper to disclose.
Figures






References
-
- Jacobs J.P., Mavroudis C., Quintessenza J.A., et al. Reoperations for pediatric and congenital heart disease: an analysis of the Society of Thoracic Surgeons (STS) congenital heart surgery database. Semin Thorac Cardiovasc Surg Pediatr Card Surg Annu. 2014;17(1):2–8. doi: 10.1053/j.pcsu.2014.01.006. - DOI - PMC - PubMed
-
- Mayer Je, Mayer J.E. Uses of homograft conduits for right ventricle to pulmonary artery connections in the neonatal period. Semin Thorac Cardiovasc Surg. 1995;7(3):130–132. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
