

Exploring the Economic Burden of Pulmonary Arterial Hypertension and Its Relation to Disease Severity and Treatment Escalation: A Systematic Literature Review
- PMID: 40244370
- PMCID: PMC12167309
- DOI: 10.1007/s40273-025-01492-1
Exploring the Economic Burden of Pulmonary Arterial Hypertension and Its Relation to Disease Severity and Treatment Escalation: A Systematic Literature Review
Erratum in
-
Correction: Exploring the Economic Burden of Pulmonary Arterial Hypertension and Its Relation to Disease Severity and Treatment Escalation: A Systematic Literature Review.Pharmacoeconomics. 2025 Jul 10. doi: 10.1007/s40273-025-01518-8. Online ahead of print. Pharmacoeconomics. 2025. PMID: 40637972 No abstract available.
Abstract
Background: Pulmonary arterial hypertension (PAH) is a highly progressive disease characterized by luminal narrowing of the pulmonary arteries, leading to progressive dyspnoea and restricted functional capacity, which can ultimately result in right ventricular failure and death. Treatment goals include improving functional class and walk distance, recovering right ventricular function, halting disease progression, and improving survival. PAH carries a high mortality rate, and treatment escalation is a common feature of disease management. Due to the substantial impact of PAH, a high economic burden has been observed. A systematic literature review (SLR) was carried out to assess the contemporary economic burden of PAH, including the impact of disease severity and treatment escalation.
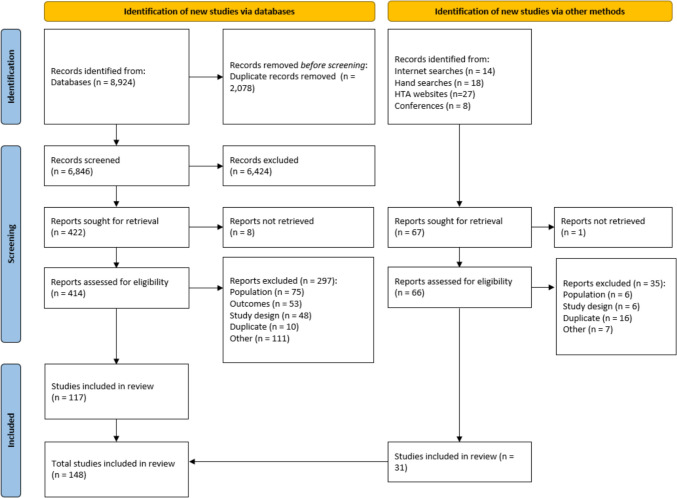
Methods: An electronic database search was conducted and supplemented with a hand search of health technology assessments and conference materials. Studies were included from 2012 to 2024, with no restrictions on geographical location. The inclusion criteria specified that adult patients with PAH (≥ 18 years) and only English language studies were captured.
Results: The review included 148 studies and evaluations, 110 of which were observational studies, 14 were economic evaluations, and 24 were health technology assessments. The studies identified reported on several healthcare resource utilization (HCRU) outcomes including hospitalization, PAH-related hospitalization, inpatient visits, emergency department (ED) visits, intensive care unit (ICU) visits, and outpatient visits. Cost data were also reported, including total costs and costs for each of the above-mentioned types of HCRU, as well as specific costs such as pharmacy and drug costs. The results provide an overview of the high economic burden caused by PAH, indicating that the economic burden increases with increasing severity; reported mean monthly costs were as high as US $14,614 (cost converted to USD 2024) for the highest severity group. These data also demonstrated the impact of PAH-specific therapies in reducing HCRU, with efficacious treatment shifting management from an inpatient to outpatient setting (i.e., reduced inpatient admissions and length of stay). Further, while treatment escalation resulted in increased pharmacy costs, this was offset by a reduction in HCRU, including hospitalizations and ED visits. Timely diagnosis was also associated with reduced economic burden, as patients with a longer delay prior to diagnosis reported a higher mean number of monthly hospitalizations, ICU stays, and ED visits. Functional limitation is a common feature of PAH disease progression and can severely impact a patient's ability to work. This SLR identified few studies that investigated such outcomes as well as broader indirect costs, such as out-of-pocket costs and productivity loss.
Discussion: This study highlights the considerable economic burden associated with PAH, which is particularly evident for HCRU, and the importance of effective disease management in reducing this burden. Additionally, these findings demonstrate the economic value of treatment escalation and suggest higher drug costs can potentially be offset through improved patient outcomes and associated reductions in HCRU.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Funding: This study was funded by Merck Sharp and Dohme LLC, a subsidiary of Merck and Co., Inc., Rahway, NJ, USA (who manufacture sotatercept). Conflict of interest: The authors disclose the following: this study was funded by Merck Sharp and Dohme LLC, a subsidiary of Merck and Co., Inc., Rahway, NJ, USA (who manufacture sotatercept). V.B. and H.B. are employees of Merck Sharp and Dohme LLC, a subsidiary of Merck and Co., Inc., Rahway, NJ, USA and may hold stock or stock options in Merck and Co., Inc., Rahway, NJ, USA. G.R. has received consulting fees from Merck and Co., Inc. and research funding from United Therapeutics. D.B., I.Z., and A.C.H. are employees of Adelphi Values PROVETM and were contracted by Merck Sharp and Dohme LLC, a subsidiary of Merck and Co., Inc., Rahway, NJ, USA, to carry out the study and to support with medical writing. Ethics approval and consent to participate: Not applicable. Consent for publication: Not applicable. Availability of data and materials: The datasets supporting the conclusions of this article are included within the article or supplementary material. The full datasets generated and analyzed during the current study are available from the corresponding author on reasonable request. Author contributions: All authors attest that they meet the ICMJE criteria for authorship. G.R. was involved in the interpretation of the data and the critical revision of the manuscript. V.B., H.B., and D.L. were involved in the study conception and design, data analysis, and critical revision of the manuscript. I.Z. and A.C.H. were involved in the study conception and design, data collection and analysis, and preparation and editing of the manuscript. D.B. was involved in the data collection and analysis and preparation and editing of the manuscript. All authors have read and approved the final manuscript.
Figures
Similar articles
-
[Volume and health outcomes: evidence from systematic reviews and from evaluation of Italian hospital data].Epidemiol Prev. 2013 Mar-Jun;37(2-3 Suppl 2):1-100. Epidemiol Prev. 2013. PMID: 23851286 Italian.
-
A rapid and systematic review of the clinical effectiveness and cost-effectiveness of topotecan for ovarian cancer.Health Technol Assess. 2001;5(28):1-110. doi: 10.3310/hta5280. Health Technol Assess. 2001. PMID: 11701100
-
Intravenous magnesium sulphate and sotalol for prevention of atrial fibrillation after coronary artery bypass surgery: a systematic review and economic evaluation.Health Technol Assess. 2008 Jun;12(28):iii-iv, ix-95. doi: 10.3310/hta12280. Health Technol Assess. 2008. PMID: 18547499
-
Signs and symptoms to determine if a patient presenting in primary care or hospital outpatient settings has COVID-19.Cochrane Database Syst Rev. 2022 May 20;5(5):CD013665. doi: 10.1002/14651858.CD013665.pub3. Cochrane Database Syst Rev. 2022. PMID: 35593186 Free PMC article.
-
What is the value of routinely testing full blood count, electrolytes and urea, and pulmonary function tests before elective surgery in patients with no apparent clinical indication and in subgroups of patients with common comorbidities: a systematic review of the clinical and cost-effective literature.Health Technol Assess. 2012 Dec;16(50):i-xvi, 1-159. doi: 10.3310/hta16500. Health Technol Assess. 2012. PMID: 23302507 Free PMC article.
References
-
- Waxman AB. Exercise physiology and pulmonary arterial hypertension. Prog Cardiovasc Dis. 2012;55(2):172–9. - PubMed
-
- Matura LA, McDonough A, Carroll DL. Cluster analysis of symptoms in pulmonary arterial hypertension: a pilot study. Eur J Cardiovasc Nurs. 2012;11(1):51–61. - PubMed
-
- Humbert M, Sitbon O, Simonneau G. Treatment of pulmonary arterial hypertension. N Engl J Med. 2004;351(14):1425–36. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
