

The red blood cell distribution width is associated with all-cause and cardiovascular mortality among individuals with non-alcoholic fatty liver disease
- PMID: 40245046
- PMCID: PMC12005546
- DOI: 10.1371/journal.pone.0321789
The red blood cell distribution width is associated with all-cause and cardiovascular mortality among individuals with non-alcoholic fatty liver disease
Abstract
Background: Identifying reliable prognostic indicators is essential for the appropriate management of non-alcoholic fatty liver disease (NAFLD). Red blood cell distribution width (RDW) has been established as an inflammatory marker associated with cardiovascular outcomes. This study aimed to evaluate the association between RDW and both cardiovascular and all-cause mortality in individuals with NAFLD.
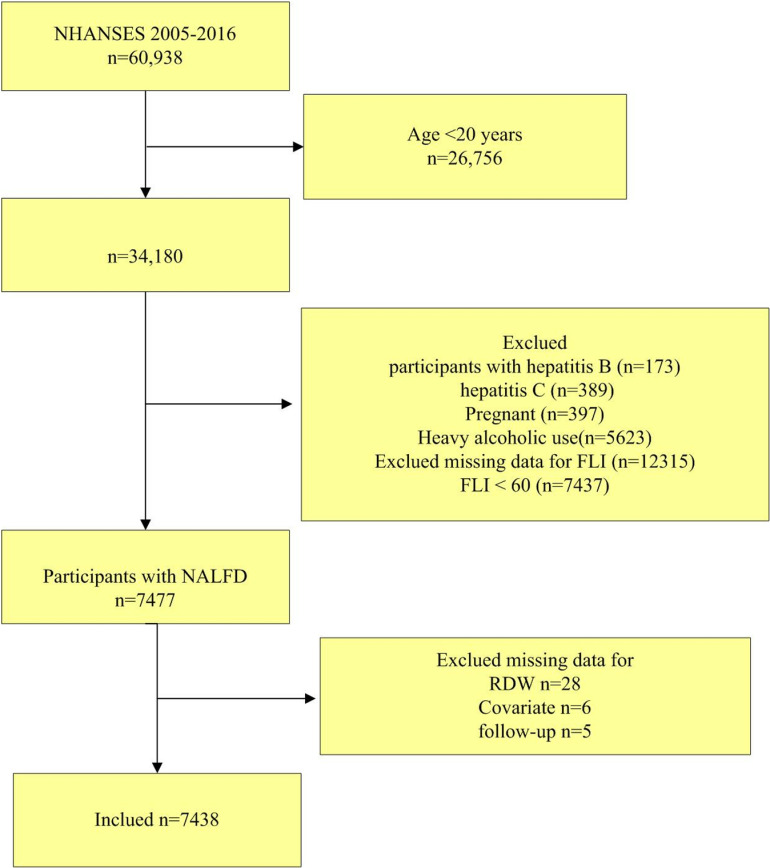
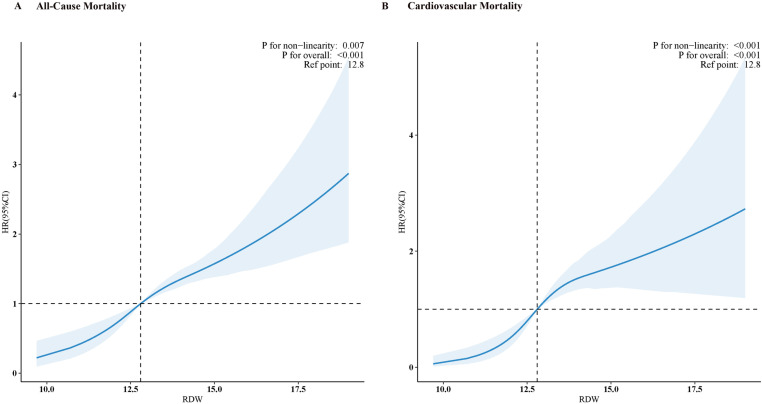
Methods: Data from 7,438 participants with NAFLD were analyzed, collected between 2005 and 2016 through the National Health and Nutrition Examination Survey (NHANES). Mortality data were retrieved from the National Death Index (NDI). Restricted cubic spline (RCS) analysis was used to illustrate the relationship between RDW and mortality risk, Weighted Cox proportional hazards models were used to assess the independent relationship between RDW and mortality risk. Receiver operating characteristic (ROC) curves were generated to evaluate the predictive ability of RDW for survival outcomes.
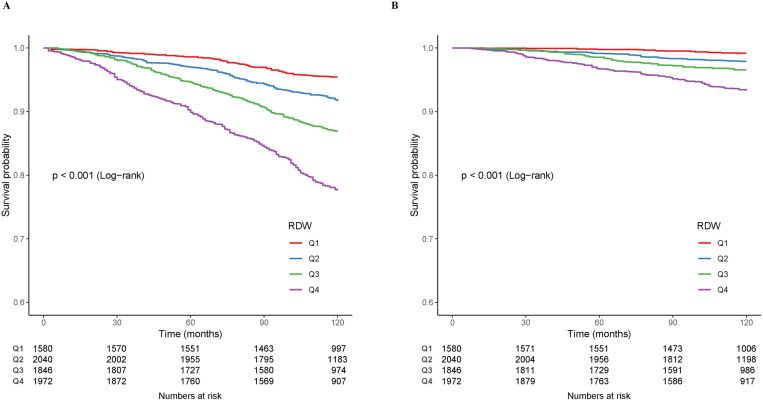
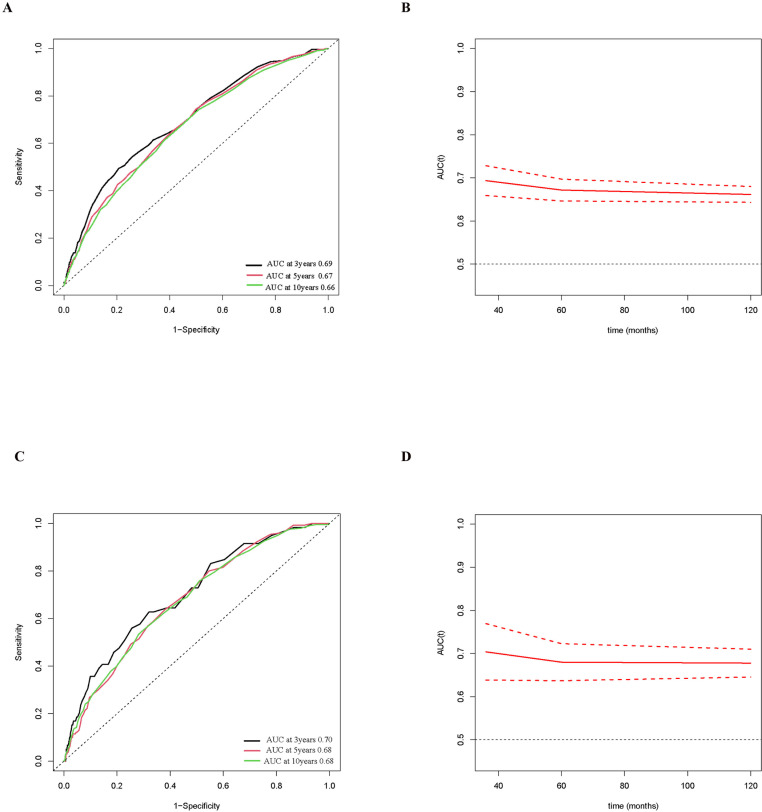
Results: During a median follow-up period of 124 months, 1,269 deaths were recorded, including 335 from cardiovascular causes. RDW positively correlated with both cardiovascular and all-cause mortality according to the RCS analysis. Participants were categorized into quartiles based on RDW levels. Those in the highest RDW quartile (Q4) demonstrated a significantly higher risk of cardiovascular mortality (HR 3.61, 95% confidence interval [CI]:2.17-6.02, P=0.009) and all-cause mortality (HR 2.29, 95% CI:1.72-3.06, P < 0.0001), according to the weighted Cox hazards models. Additionally, the area under the curve (AUC) for all-cause mortality at 3, 5 and 10 years was, 0.69, 0.67, and 0.66, respectively. For cardiovascular mortality, the AUCs were 0.70, 0.68, and 0.68, respectively.
Conclusion: Among patients with NAFLD, RDW was identified as an independent predictor of increased cardiovascular and all-cause mortality risk.
Copyright: © 2025 Huang et al. This is an open access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
Similar articles
-
Predictive role of red blood cell distribution width and hemoglobin-to-red blood cell distribution width ratio for mortality in patients with COPD: evidence from NHANES 1999-2018.BMC Pulm Med. 2024 Aug 26;24(1):413. doi: 10.1186/s12890-024-03229-w. BMC Pulm Med. 2024. PMID: 39187816 Free PMC article.
-
Association of blood cadmium levels with all-cause and cause-specific mortality among adults with non-alcoholic fatty liver disease: a prospective cohort study.Front Public Health. 2025 Apr 4;13:1573760. doi: 10.3389/fpubh.2025.1573760. eCollection 2025. Front Public Health. 2025. PMID: 40255375 Free PMC article.
-
Red cell distribution width and risk of cardiovascular mortality: Insights from National Health and Nutrition Examination Survey (NHANES)-III.Int J Cardiol. 2017 Apr 1;232:105-110. doi: 10.1016/j.ijcard.2017.01.045. Epub 2017 Jan 6. Int J Cardiol. 2017. PMID: 28117138
-
Red cell distribution width and mortality in older adults: a meta-analysis.J Gerontol A Biol Sci Med Sci. 2010 Mar;65(3):258-65. doi: 10.1093/gerona/glp163. Epub 2009 Oct 30. J Gerontol A Biol Sci Med Sci. 2010. PMID: 19880817 Free PMC article. Review.
-
The prognostic value of red blood cell distribution width for mortality in intracranial hemorrhage: A systematic review and meta-analysis.Medicine (Baltimore). 2025 Mar 14;104(11):e41487. doi: 10.1097/MD.0000000000041487. Medicine (Baltimore). 2025. PMID: 40101061 Free PMC article.
References
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
