

Prevalence of endometriosis in Mayer-Rokitansky-Küster-Hauser syndrome variants: a systematic review and meta-analysis
- PMID: 40246293
- PMCID: PMC12127514
- DOI: 10.1093/humrep/deaf057
Prevalence of endometriosis in Mayer-Rokitansky-Küster-Hauser syndrome variants: a systematic review and meta-analysis
Abstract
Study question: In patients with Mayer-Rokitansky-Küster-Hauser syndrome (MRKHS; population), is the presence of functional endometrium (FE) in uterine remnants (URs) (exposure), compared with the absence of FE in UR/absence of UR (comparison), associated with a higher prevalence of endometriosis (outcome)?
Summary answer: The aggregate prevalence of endometriosis was considerably higher in MRKHS patients with FE (MRKHSFE+) than in those without FE (MRKHSFE-).
What is known already: The pathogenesis of endometriosis is not fully understood. The finding of pelvic endometriosis in patients with MRKHS is one of the main objections to the retrograde menstruation (RM) hypothesis. The recent advent of high-resolution ultrasonography and magnetic resonance imaging (MRI) allowed the reliable preoperative identification of FE concealed within UR, and histopathological examination after UR removal is no longer the only means of verifying the presence of a mucosal component. A similar prevalence of endometriosis in MRKHSFE+ and MRKHSFE- patients, as assessed by preoperative ultrasound (US) and/or MRI, would essentially rule out the RM/implantation theory, whereas a substantially higher prevalence of endometriosis in MRKHSFE+ than in MRKHSFE- patients would challenge the embryonic remnants/coelomic metaplasia hypothesis.
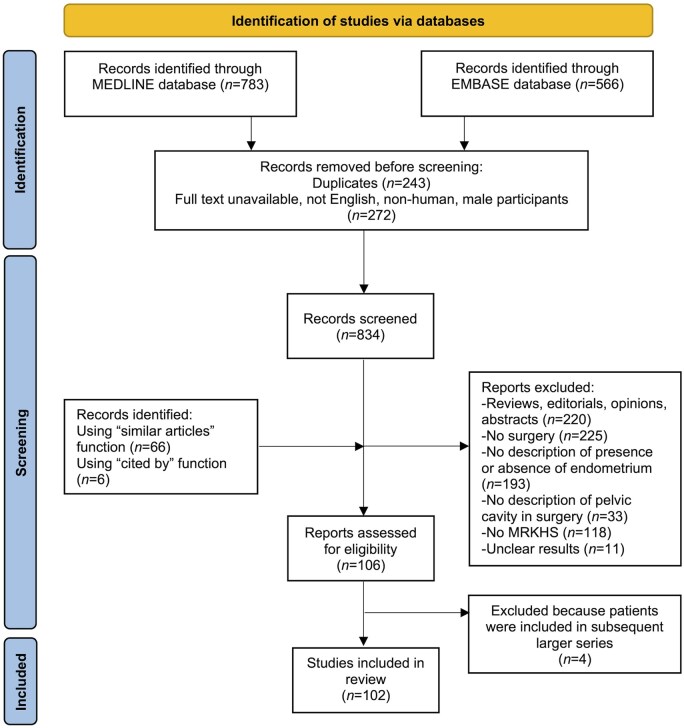
Study design, size, duration: This systematic review was restricted to full-length, English-language articles published in peer-reviewed journals between 1 January 1980 and 1 June 2024. The electronic PubMed and Embase databases were searched in June 2024. The keyword 'endometriosis' was used in combination with 'Mayer-Rokitansky-Küster-Hauser syndrome', 'Müllerian agenesis', 'uterine agenesis', 'vaginal agenesis', 'Müllerian anomalies', and 'female genital malformations'. References from relevant publications were screened, and PubMed's 'similar articles' and 'cited by' functions were used.
Participants/materials, setting, methods: Studies were selected if they reported the presence or absence of FE within UR investigated by preoperative US or MRI or histology after surgical removal, and the presence or absence of surgically confirmed endometriosis. Case series and case reports were deemed eligible for inclusion. Studies not specifically stating the intent to search for the presence of endometrium within UR, or not reporting the results of ultrasonography or MRI, or histological examinations were excluded. Two reviewers independently abstracted data. The risk of bias was assessed using a tool specifically devised to ascertain the methodological quality of case series and case reports.
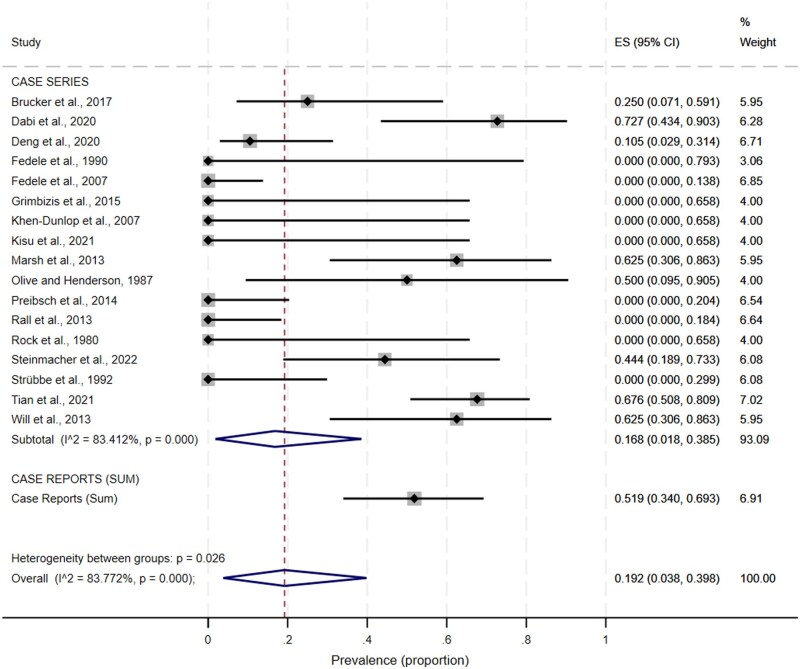
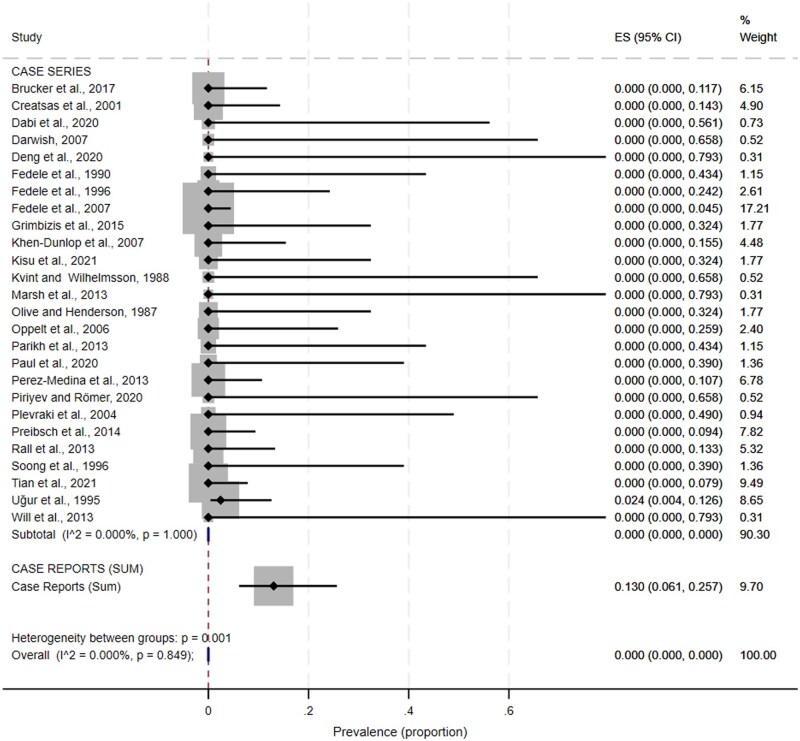
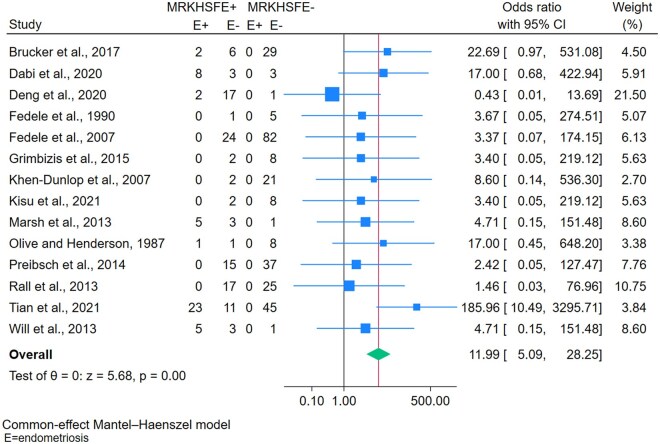
Main results and the role of chance: A total of 102 studies (29 case series and 73 case reports), comprising 666 MRKHS patients in whom the presence or absence of FE was verified were included. Endometriosis was detected in 71 participants (10.7%; 95% CI, 8.5-13.2%), and its prevalence was 8.6% (51/593; 95% CI, 6.6-11.2%) in case series and 27.4% (20/73; 95% CI, 18.4-38.6%) in case reports (P<0.0001). When considering only the 19 case series with ≥10 participants, the proportion of MRKHS patients with endometriosis was 3.4% (41/1219; 95% CI, 2.5-4.5%). Among the 71 MRKHS patients with endometriosis, 64 had coexisting FE, and only seven had no evidence of FE within UR or did not have UR. The proportion of patients with endometriosis was 32.0% in the subgroup with FE (64/200; 95% CI, 25.9-38.8%) and 1.5% (7/466; 95% CI, 0.7-3.1%) in the subgroup without FE within UR/without UR. At meta-analysis considering case series, the overall prevalence estimates of endometriosis in patients with and without FE were, respectively, 16.8% (95% CI, 1.8-38.5%) and 0% (95% CI, 0-0%). In order to evaluate the association between FE and endometriosis we also conducted a meta-analysis that included case series reporting both FE+ and FE- patients. A significantly increased risk of endometriosis was observed in MRKHSFE+ patients compared with MRKHSFE- patients (overall odds ratio estimate was 12.0; 95% CI, 5.1-28.3%). The quality of the evidence score was higher in the case series subgroup (median score, 4 points; interquartile range, 3-5 points) than in the case reports subgroup (median score, 3 points; interquartile range, 2-4 points).
Limitations, reason for caution: Due to the uncontrolled and non-experimental study design, case series and case reports are associated with an increased risk of selection, performance, detection, attrition, and reporting bias. In the seven cases of endometriosis in patients purportedly without detected FE, a preoperative MRI was not systematically performed or erroneous findings were reported, the anatomical description at surgery was incomplete or inconsistent, the histopathological diagnosis of endometriosis was missing or questionable, and precise microscopic features were not always described. Whether FE (exposure) was truly absent in all these cases and/or whether all lesions diagnosed as endometriosis (outcome) were indeed true disease, seems uncertain.
Wider implications of the findings: Our findings should raise awareness of the importance of accurately assessing and reporting the presence or absence of FE within UR, and of systematically performing biopsies of visually diagnosed endometriosis in MRKHS patients. Considering the high risk of bias, the detection of endometriosis in MRKHS patients allegedly without FE in the few relevant case reports published in the last four decades should no longer be interpreted tout court as proof for the coelomic metaplasia/embryonic remnants theory.
Study funding/competing interest(s): No funding was received for this review. P.Ve. is a member of the Editorial Board of Human Reproduction Open, the Journal of Obstetrics and Gynaecology Canada, and the International Editorial Board of Acta Obstetricia et Gynecologica Scandinavica; has received royalties from Wolters Kluwer for chapters on endometriosis management in the clinical decision support resource UpToDate; and maintains both a public and private gynaecological practice. E.S. is Editor-in-Chief of Human Reproduction Open; discloses payments from Ferring for research grants and honoraria from Merck-Serono for lectures; and maintains both a public and private gynaecological practice. P.Vi. is Co-Editor-in-Chief of Journal of Endometriosis and Uterine Disorders. All other authors declare they have no conflict of interest.
Registration number: The study protocol was registered on PROSPERO (registration number, CRD42024512351).
Keywords: Mayer–Rokitansky–Küster–Hauser syndrome; Müllerian anomalies; coelomic metaplasia; embryonic remnants; endometriosis; infertility; pathogenesis; retrograde menstruation; uterine agenesis; vaginal agenesis.
© The Author(s) 2025. Published by Oxford University Press on behalf of European Society of Human Reproduction and Embryology.
Conflict of interest statement
P.Ve. is a member of the Editorial Board of Human Reproduction Open, the Journal of Obstetrics and Gynaecology Canada, and of the International Editorial Board of Acta Obstetricia et Gynecologica Scandinavica; has received royalties from Wolters Kluwer for chapters on endometriosis management in the clinical decision support resource UpToDate; and maintains both a public and private gynaecological practice. E.S. is Editor-in-Chief of Human Reproduction Open; discloses payments from Ferring for research grants and honoraria from Merck-Serono for lectures; and maintains both a public and private gynaecological practice. P.Vi. is Co-Editor-in-Chief of Journal of Endometriosis and Uterine Disorders. All other authors declare they have no conflict of interest.
Figures
References
-
- Acién P. Endometriosis and genital anomalies: some histogenetic aspects of external endometriosis. Gynecol Obstet Invest 1986;22:102–107. - PubMed
-
- Acién P, Lloret M, Chehab H. Endometriosis in a patient with Rokitansky–Kuster–Hauser syndrome. Gynecol Obstet Invest 1988;25:70–72. - PubMed
-
- Albahlol IA, Elshamy M, El-Hady HAF, Abd-Elwahab EM. Leiomyomas in a case of Mayer–Rokitansky–Kuster–Hauser syndrome: case report. Eur J Obstet Gynecol Reprod Biol 2020;244:199–200. - PubMed
