

Telehealth Support From Cardiologists to Primary Care Physicians in Heart Failure Treatment: Mixed Methods Feasibility Study of the Brazilian Heart Insufficiency With Telemedicine Trial
- PMID: 40246296
- PMCID: PMC12046267
- DOI: 10.2196/64438
Telehealth Support From Cardiologists to Primary Care Physicians in Heart Failure Treatment: Mixed Methods Feasibility Study of the Brazilian Heart Insufficiency With Telemedicine Trial
Abstract
Background: Heart failure is a prevalent condition ideally managed through collaboration between health care sectors. Telehealth between cardiologists and primary care physicians is a strategy to improve the quality of care for patients with heart failure. Still, the effectiveness of this approach on patient-relevant outcomes needs to be determined.
Objective: This study aimed to assess the feasibility of telehealth support provided by cardiologists for treating patients with heart failure to primary care physicians from public primary care practices in Rio de Janeiro, Brazil.
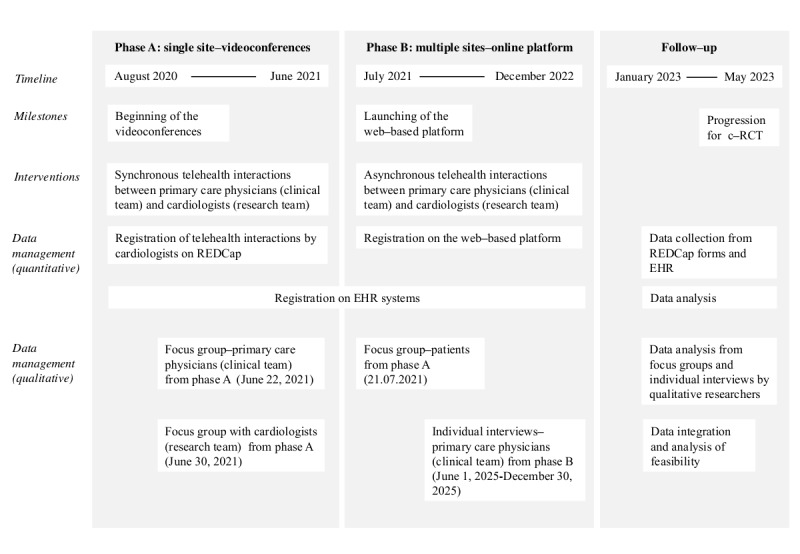
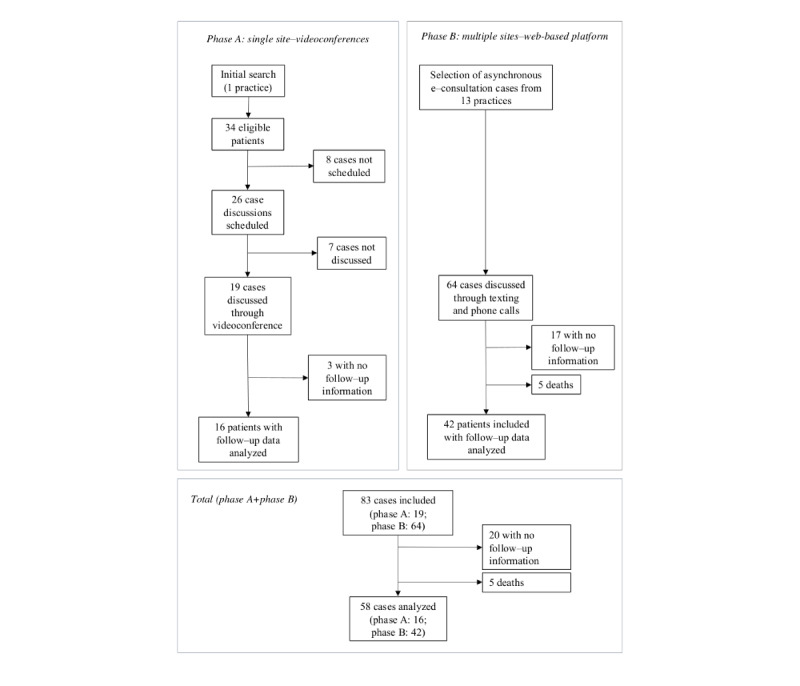
Methods: We used mixed methods to assess the feasibility of telehealth support. From 2020 to 2022, we tested 2 telehealth approaches: synchronous videoconferences (phase A) and interaction through an asynchronous web platform (phase B). The primary outcome was feasibility. Exploratory outcomes were telehealth acceptability of patients, primary care physicians, and cardiologists; the patients' clinical status; and prescription practices. Qualitative methods comprised content analysis of 3 focus groups and 15 individual interviews with patients, primary care physicians, and cardiologists. Quantitative methods included the baseline assessment of 83 patients; a single-arm, before-and-after assessment of clinical status in 58 patients; and an assessment of guideline-directed medical therapy in 28 patients with reduced ejection fraction measured within 1 year of follow-up. We integrated qualitative and quantitative data using a joint display table and used the A Process for Decision-Making After Pilot and Feasibility Trials framework for feasibility assessment.
Results: Telehealth support from cardiologists to primary care physicians was generally well accepted. As barriers, patients expressed concern about reduced direct access to cardiologists, primary care physicians reported work overload and a lack of relative advantage, and cardiologists expressed concern about the sustainability of the intervention. Quantitative analysis revealed an overall poor baseline clinical status of patients with heart failure, with 53% (44/83) decompensated, as expected. Compliance with guideline-directed medical therapy for the treatment of heart failure with reduced ejection fraction after telehealth showed a modest improvement for β-blockers (17/20, 85% to 18/19, 95%) and renin-angiotensin-aldosterone system inhibitors (14/20, 70% to 15/19, 79%) but a drop in the prescription of spironolactone (16/20, 80% to 15/20, 75%). Neprilysin and sodium-glucose cotransporter 2 inhibitors were introduced in 4 and 1 patient, respectively. Missing record data precluded a more precise analysis. The feasibility assessment was positive, favoring the asynchronous modality. Potential modifications include more effective patient and professional recruitment strategies and educational activities to raise awareness of collaborative support in primary care.
Conclusions: Telehealth was feasible to implement. Considering the stakeholders' views and insights on the process is paramount to attaining engagement. Missing data must be anticipated for future research in this setting. Considering the recommended adaptations, the intervention can be studied in a cluster-randomized trial.
Keywords: family practice; heart failure; intersectoral collaboration; low- and middle-income countries; primary health care; telehealth; telemedicine.
©Leonardo Graever, Priscila Cordeiro Mafra, Vinicius Klein Figueira, Vanessa Navega Miler, Júlia dos Santos Lima Sobreiro, Gabriel Pesce de Castro da Silva, Aurora Felice Castro Issa, Leonardo Cançado Monteiro Savassi, Mariana Borges Dias, Marcelo Machado Melo, Viviane Belidio Pinheiro da Fonseca, Isabel Cristina Pacheco da Nóbrega, Maria Kátia Gomes, Laís Pimenta Ribeiro dos Santos, José Roberto Lapa e Silva, Anne Froelich, Helena Dominguez. Originally published in JMIR Cardio (https://cardio.jmir.org), 17.04.2025.
Conflict of interest statement
Conflicts of Interest: None declared.
Figures
Similar articles
-
Telemedicine Support for Primary Care Providers versus Usual Care in Patients with Heart Failure: Protocol of a Pragmatic Cluster Randomised Trial within the Brazilian Heart Insufficiency with Telemedicine (BRAHIT) Study.Int J Environ Res Public Health. 2023 May 24;20(11):5933. doi: 10.3390/ijerph20115933. Int J Environ Res Public Health. 2023. PMID: 37297537 Free PMC article.
-
The future of Cochrane Neonatal.Early Hum Dev. 2020 Nov;150:105191. doi: 10.1016/j.earlhumdev.2020.105191. Epub 2020 Sep 12. Early Hum Dev. 2020. PMID: 33036834
-
A Hospital-Community-Family-Based Telehealth Program for Patients With Chronic Heart Failure: Single-Arm, Prospective Feasibility Study.JMIR Mhealth Uhealth. 2019 Dec 13;7(12):e13229. doi: 10.2196/13229. JMIR Mhealth Uhealth. 2019. PMID: 31833835 Free PMC article. Clinical Trial.
-
Healthcare stakeholders' perceptions and experiences of factors affecting the implementation of critical care telemedicine (CCT): qualitative evidence synthesis.Cochrane Database Syst Rev. 2021 Feb 18;2(2):CD012876. doi: 10.1002/14651858.CD012876.pub2. Cochrane Database Syst Rev. 2021. PMID: 33599282 Free PMC article.
-
Current experience and future potential of facilitating access to digital NHS primary care services in England: the Di-Facto mixed-methods study.Health Soc Care Deliv Res. 2024 Sep;12(32):1-197. doi: 10.3310/JKYT5803. Health Soc Care Deliv Res. 2024. PMID: 39324475 Review.
References
-
- Reeves S, Pelone F, Harrison R, Goldman J, Zwarenstein M. Interprofessional collaboration to improve professional practice and healthcare outcomes. Cochrane Database Syst Rev. 2017 Jun 22;6(6):CD000072. doi: 10.1002/14651858.CD000072.pub3. https://europepmc.org/abstract/MED/28639262 - DOI - PMC - PubMed
-
- Bashshur R, Shannon G, Krupinski E, Grigsby J. The taxonomy of telemedicine. Telemed J E Health. 2011;17(6):484–94. doi: 10.1089/tmj.2011.0103. http://hdl.handle.net/2027.42/90498 - DOI - PubMed
-
- WHO guideline recommendations on digital interventions for health system strengthening. World Health Organization. [2024-04-29]. https://apps.who.int/iris/handle/10665/357828 . - PubMed
-
- Liddy C, Moroz I, Mihan A, Nawar N, Keely E. A systematic review of asynchronous, provider-to-provider, electronic consultation services to improve access to specialty care available worldwide. Telemed J E Health. 2019 Mar;25(3):184–98. doi: 10.1089/tmj.2018.0005. https://www.liebertpub.com/doi/10.1089/tmj.2018.0005 - DOI - DOI - PubMed
-
- Blank L, Baxter S, Woods HB, Goyder E, Lee A, Payne N, Rimmer M. Referral interventions from primary to specialist care: a systematic review of international evidence. Br J Gen Pract. 2014 Dec 01;64(629):e765–74. doi: 10.3399/bjgp14x682837. https://bjgp.org/lookup/doi/10.3399/bjgp14X682837 - DOI - DOI - PMC - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
