

Reduced venetoclax exposure to 7 days vs standard exposure with hypomethylating agents in newly diagnosed AML patients
- PMID: 40246832
- PMCID: PMC12006504
- DOI: 10.1038/s41408-025-01269-x
Reduced venetoclax exposure to 7 days vs standard exposure with hypomethylating agents in newly diagnosed AML patients
Abstract
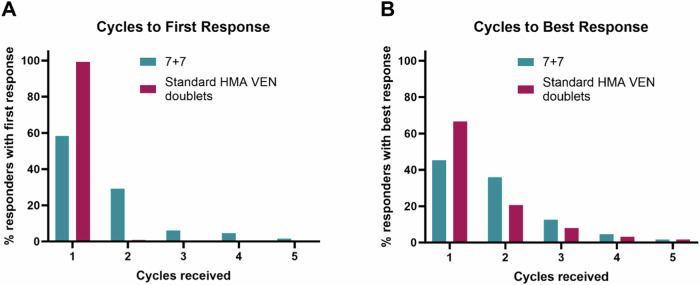
Hypomethylating agent (HMA) plus venetoclax (VEN) regimens are standard of care in patients with acute myeloid leukemia (AML) ineligible for intensive chemotherapy. While the VEN label recommends continuous 28-day cycles, shortened VEN durations may induce similar response rates and improve tolerability. It is unknown how a VEN exposure reduced to 7 days during cycles compares to standard HMA + VEN. We retrospectively compared newly diagnosed AML patients treated with azacitidine (AZA) x 7 days plus VEN x 7 days ("7 + 7" regimen) from the first cycle (n = 82) vs patients treated with standard dose HMA + VEN (std-HMA/VEN) (n = 166). Composite complete remission rate was similar between cohorts (72% vs 72%; p = 0.95) and a median number of cycles to best response was 2 with "7 + 7" vs 1 with std-HMA/VEN (p = 0.03). Concerning toxicity, platelet transfusion rates during cycle 1 as well as early mortality at 8-weeks (6% vs 16%; p = 0.03) were lower in "7 + 7" cohort. Finally, the median OS was 11.2 months (2-year 28%) with "7 + 7" vs 10.3 months (2-year 34%) with "std-HMA/VEN" (p = 0.75). In summary, acknowledging limitations of a retrospective comparison, a shortened course of VEN used for 7 days every 28 days resulted in similar response rates and survival when compared to standard VEN exposure.
© 2025. The Author(s).
Conflict of interest statement
Competing interests: CW: Consultant/Advisory Boards: BMS, Abbvie. NG: Consultant/Advisory Boards: BMS. JBM: Honoraria: Jazz Pharmaceuticals, Astellas Pharma, SERVIER. Consultant/Advisory Boards: AbbVie, Gilead Sciences. Travel, Accommodations, Expenses: AbbVie. CM: Research funding: Incyte. LP: Consultant/Advisory Boards: Janssen, Takeda, Abbvie, Gilead, Kephren and Résilience. SDB: Consultant/Advisory Boards: Servier, BMS, GSK, Syndax Pharmaceuticals, and Remix Therapeutics. Honoraria from BMS, AbbVie, Servier, Jazz Pharmaceuticals, Astellas, and Loxo Oncology. Speakers’ bureau: Servier, BMS, Jazz Pharmaceuticals, Astellas, and AbbVie. Research funding: Forma Therapeutics and Auron Therapeutics. CD: Consultant/Advisory Boards: Abbvie, AstraZeneca, Astellas, BMS, Genentech, GenMab, GSK, ImmuneOnc, Notable Labs, Rigel, Schrodinger, Servier. CDD is supported by the LLS Scholar in Clinical Research Award. ABazinet, SC, ABataller, JD, NA, BC, CR, DL, AM, NS, SB, KS, SKH, MS, FP, DRW, ND, TK, DB, FR, AP and HK had no conflict of interest.
Figures



References
-
- Döhner H, Wei AH, Appelbaum FR, Craddock C, DiNardo CD, Dombret H, et al. Diagnosis and management of AML in adults: 2022 recommendations from an international expert panel on behalf of the ELN. Blood. 2022;140:1345–77. - PubMed
-
- DiNardo CD, Jonas BA, Pullarkat V, Thirman MJ, Garcia JS, Wei AH, et al. Azacitidine and Venetoclax in Previously Untreated Acute Myeloid Leukemia. N. Engl J Med. 2020;383:617–29. - PubMed
-
- Pratz KW, DiNardo CD, Selleslag D, Li J, Yamamoto K, Konopleva M, et al. Postremission cytopenia management in patients with acute myeloid leukemia treated with venetoclax and azacitidine in VIALE‐A. Am J Hematol. 2022;97:E416–E419. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Research Materials
