

Finite element analysis and clinical evaluation of cross locking external fixator configuration for distal third tibia fracture
- PMID: 40247025
- PMCID: PMC12006471
- DOI: 10.1038/s41598-025-97090-4
Finite element analysis and clinical evaluation of cross locking external fixator configuration for distal third tibia fracture
Abstract
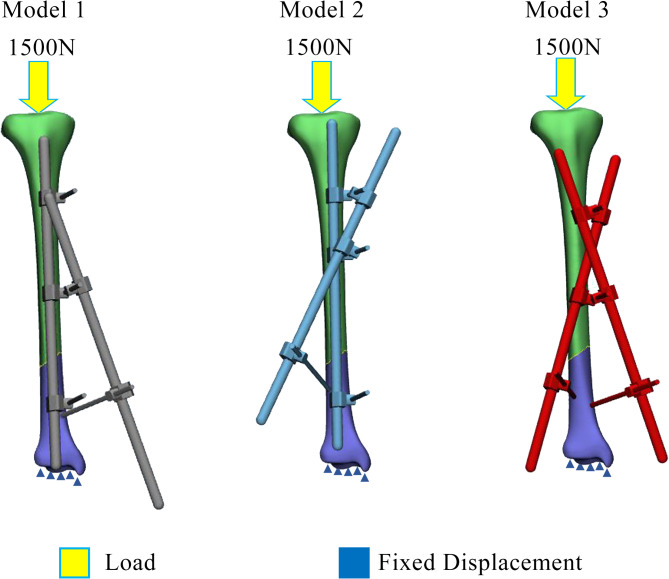
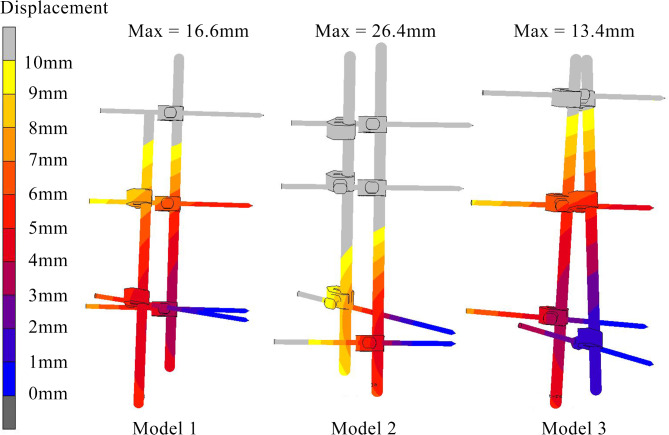
External fixators have been used effectively in damage control orthopaedic and open fractures management of various bones. It is well known that stability of external fixators is greatly influenced by its construct. Various rules have been documented to influence the stiffness and stability of external fixators. In this study, two clinical cases treated with a novel concept of cross self-locking rods external fixation construct were being described, coupled with biomechanical analysis of its stability in comparison with other constructs by using finite element study. These novel self-locking rods configuration proven improve strength by applying the same numbers of rod and pin with the delta frame construct in clinical practice. A validated three-dimensional (3D) model of the bone from a previous study was used and external fixator were designed via computer-aided design (CAD) modelling software, Solidworks. A 1500 N load representing the axial load compression during weight bearing was applied to the tibia with the distal segment of the fracture site secured without any movement. The clinical results showed bone healing process with both cases achieving bone union within the acceptable time. The results of the finite element study shows that the double cross self-locking rods construct had better stability since it showed optimum magnitude in relative micromotion (0.18 mm), lowest stress at the fracture site (189 MPa), displacement of fixator (13.4 mm), and stress at the fixator (687 MPa). In conclusion, double cross self-locking design could provide optimum stability of the external fixator construct by providing better stress distribution at the bone and external fixator, minimize displacement and micromotion at fracture fragments.
Keywords: Bone healing; Cross-locking fixator; Finite element; Micromovement; Tibia fracture.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Competing interests: The authors declare no competing interests. Institutional review board statement: The study was conducted according to the guidelines of the Declaration of Helsinki and ethically approved by National Institutes of Health, Ministry of Health Malaysia (Reference no.: NMRR-20-147-53061(IIR)). Informed consent statement: Informed consent was obtained from all subjects involved in the study. Declaration of AI use: The authors declare not use AI-assisted technologies in creating this article. Consent for publication: The authors consent for the publication of this manuscript. Transparency statement: The authors affirm that this manuscript is an honest, accurate, and transparent account of the study being reported; that no important aspects of the study have been omitted; and that any discrepancies from the study as planned (and, if relevant, registered) have been explained.
Figures






References
-
- Sen, D. Principles and overview of external fixators in orthopaedic traumatology. In Handbook of Orthopaedic Trauma Implantology 1–23 (Springer, Singapore, 2023). 10.1007/978-981-15-6278-5_16-2.
-
- Rogol, E. V. External fixation for tissue preservation following complex mandible trauma and its sequelae: Reminder of a time-honored method and case series of 23 patients. Oral Surg. Oral Med. Oral Pathol. Oral Radiol.10.1016/j.oooo.2024.10.113 (2024). - PubMed
-
- Pourabbas, B., Emad, J., Dehghani, J., Heidari, S. & Vosoughi, A. R. Mechanical evaluation of the effect of the rod to rod distance on the stiffness of uniplanar external fixator frames. Musculoskelet. Surg.107, 397–403. 10.1007/s12306-023-00782-1 (2023). - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
