

Prognostic analysis of patients with CRLM based on CRS score: a single-center retrospective study
- PMID: 40247181
- PMCID: PMC12004860
- DOI: 10.1186/s12885-025-14135-7
Prognostic analysis of patients with CRLM based on CRS score: a single-center retrospective study
Abstract
Background: To improve prognosis of patients with synchronous colorectal liver metastasis (CRLM), we constructed a nomogram model to improve outcome through risk stratification and decision support.
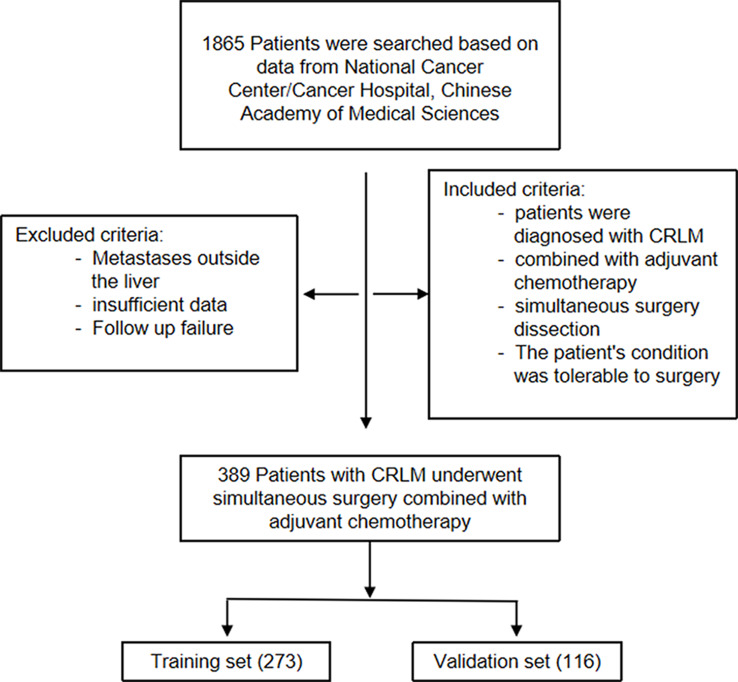
Methods: The 389 CRLM patients (273 training set and 116 validation set at a ratio of 7: 3) receiving systematic chemotherapy and synchronously resection with/without radiofrequency ablation (RFA) were retrospectively investigated. Overall survival (OS) and recurrence free survival (RFS) were mainly endpoint. A normo-gram model was conduct. The receiver operating characteristic (ROC) curve, decision curve analysis (DCA), C-index and calibration curve were performed to assess stablity and efficacy of model. The prognosis was evaluated based on Kaplan-Meier (KM) curve.
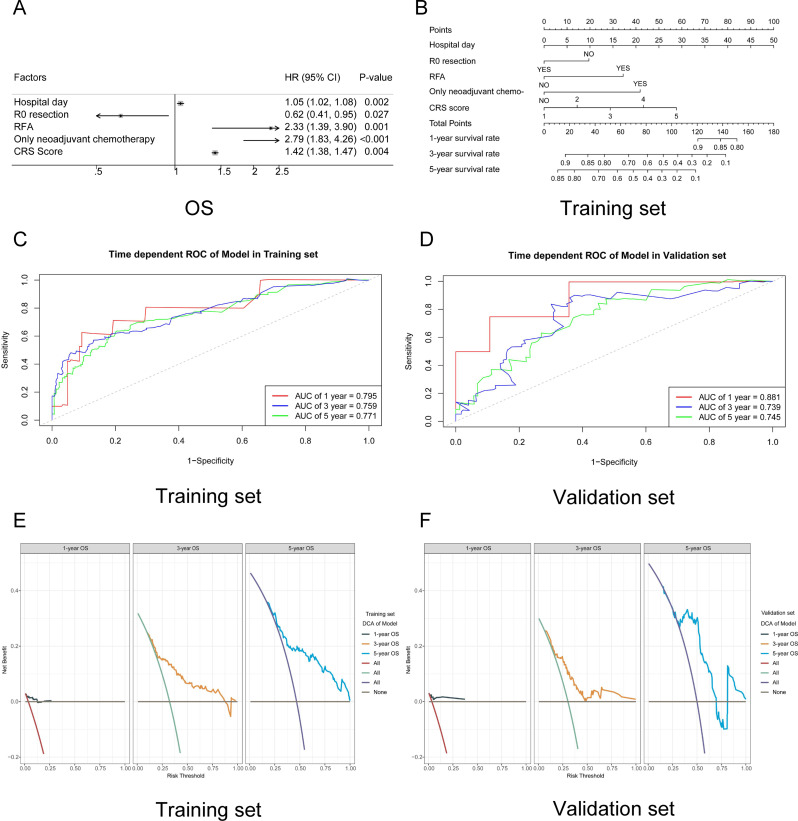
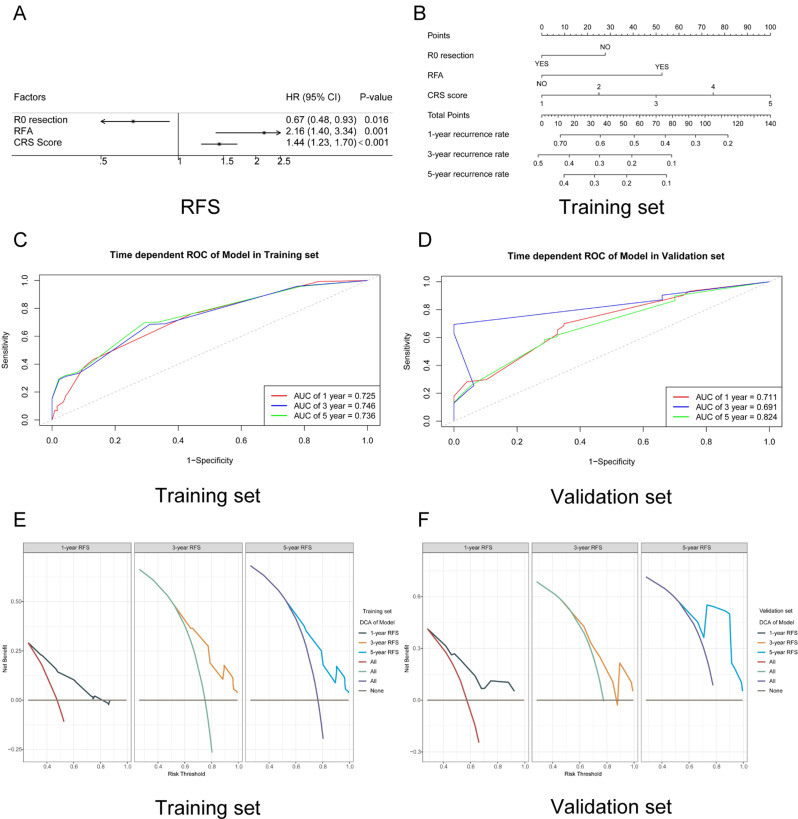
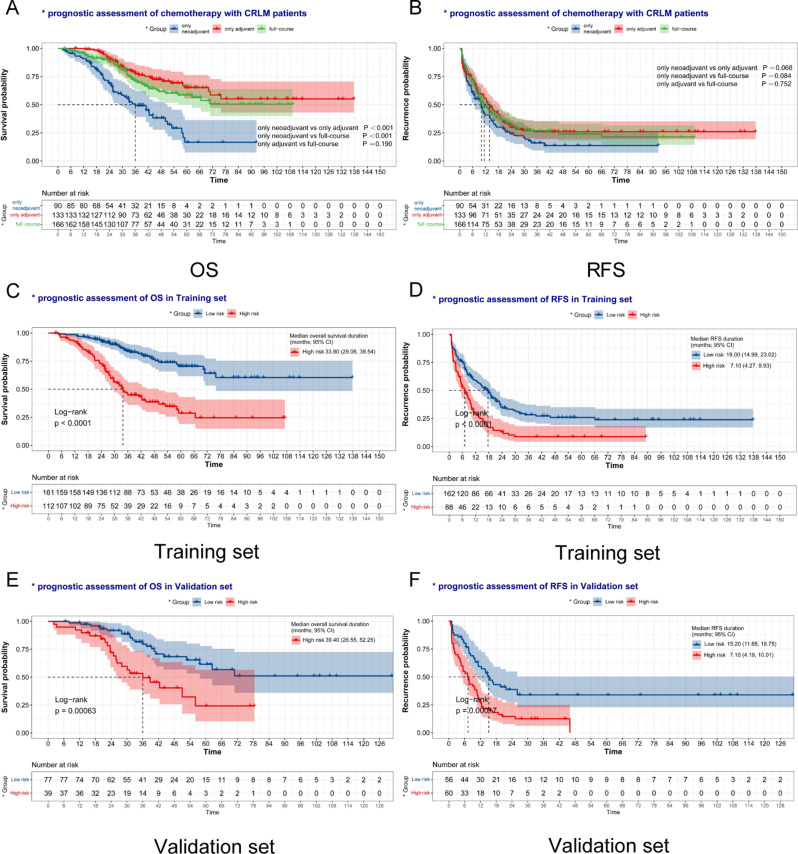
Results: A total of 389 CRLM patients were included. The median OS and RFS times were 70.20 months (95% CIs: 57.73, 82.68) and 11.70 months (95% CIs: 9.75, 13.65), respectively. These patients were divided into training set and validation set at a ratio of 7: 3. In training set, 1, 3, and 5-year survival rate of OS was 97.38%, 71.18%, and 54.56% as well as RFS was 52.57%, 22.65%, and 21.12%, respectively. Cox model showed that hospital day, R0 resection, RFA, only neoadjuvant chemotherapy and CRS score were independent prognostic factors for CRLM patients. The patients were divided into high-risk group and low-risk group based on cut-off value of score calculated by model. The KM curves were statistically different between two groups (P < 0.01). The ROC curve, DCA and calibration curve showed a good prediction efficacy. the C-index of OS and RFS were 0.72 and 0.68, respectively, which were also verified in the validation set (OS, 0.71; RFS, 0.65).
Conclusions: A good prediction model was developed and validated to assess the prognoses of CRLM patients. Systematic chemotherapy and R0 resection could benefit patients' survival and improve prognosis.
Keywords: Chemotherapy; Colorectal liver metastasis; Prognosis; Surgery.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: The study protocol, including treatment protocol and data collection, was in accordance with the Declaration of the Helsinki Association of World Medical Ethics Guidelines. Approved by the Research Ethics Committee of National Cancer Center/National Clinical Research Center for Cancer/Cancer Hospital, Chinese Academy of Medical Sciences and Peking Union Medical College and individual written informed consent for this retrospective analysis was waived. Competing interests: The authors declare no competing interests. Conflict of interest: There are no conflicts of interest to declare.
Figures
Similar articles
-
Construction and validation of "WCH-nomogram" for predicting the prognosis after resection of colorectal liver metastases.Cancer Med. 2024 May;13(9):e7222. doi: 10.1002/cam4.7222. Cancer Med. 2024. PMID: 38698687 Free PMC article.
-
Postoperative adjuvant chemotherapy is important for improving long-term survival in patients with colorectal cancer liver metastases undergoing simultaneous resection.J Gastroenterol Hepatol. 2024 May;39(5):908-919. doi: 10.1111/jgh.16504. Epub 2024 Feb 7. J Gastroenterol Hepatol. 2024. PMID: 38323685
-
Constructing a prognostic model for colorectal cancer with synchronous liver metastases after preoperative chemotherapy: a study based on SEER and an external validation cohort.Clin Transl Oncol. 2024 Dec;26(12):3169-3190. doi: 10.1007/s12094-024-03513-5. Epub 2024 Jun 4. Clin Transl Oncol. 2024. PMID: 38834909 Free PMC article.
-
Efficacy of first-line radiofrequency ablation combined with systemic chemotherapy plus targeted therapy for initially unresectable colorectal liver metastases.Int J Hyperthermia. 2025 Dec;42(1):2432988. doi: 10.1080/02656736.2024.2432988. Epub 2025 Feb 2. Int J Hyperthermia. 2025. PMID: 39894452
-
The prognosis of radiofrequency ablation versus hepatic resection for patients with colorectal liver metastases: A systematic review and meta-analysis based on 22 studies.Int J Surg. 2021 Mar;87:105896. doi: 10.1016/j.ijsu.2021.105896. Epub 2021 Feb 12. Int J Surg. 2021. PMID: 33588125
References
-
- Sung H, Ferlay J, Siegel RL, et al. Global Cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2021;71(3):209–49. - PubMed
-
- Ciardiello F, Ciardiello D, Martini G, et al. Clinical management of metastatic colorectal cancer in the era of precision medicine. CA Cancer J Clin. 2022;72(4):372–401. - PubMed
-
- Benson AB, Venook AP, Al-Hawary MM, et al. Colon cancer, version 2.2021, NCCN clinical practice guidelines in oncology. J Natl Compr Canc Netw. 2021;19(3):329–59. - PubMed
-
- Hong YS, Song SY, Lee SI, et al. A phase II trial of capecitabine in previously untreated patients with advanced and/or metastatic gastric cancer. Ann Oncol. 2004;15(9):1344–7. - PubMed
MeSH terms
Grants and funding
- SZSM202011010/Shenzhen High-level Hospital Construction Fund and Supported by Shenzhen Key Medical Discipline Construction Fund
- 81972311 & 82141127/National Natural Science Foundation of China
- SZSM202011010/Sanming Project of Medicine in Shenzhen
- 2019PT310026/the Nonprofit Central Research Institute Fund of Chinese Academy of Medical Sciences
- 2023YFC3403800 & 2023YFC3403804/National Key Research and Development Program of China
LinkOut - more resources
Full Text Sources
Medical
