

Comparative efficacy of mind-body exercise for pain, function, quality of life in knee osteoarthritis: a systematic review and network meta-analysis
- PMID: 40247321
- PMCID: PMC12004734
- DOI: 10.1186/s13018-025-05682-7
Comparative efficacy of mind-body exercise for pain, function, quality of life in knee osteoarthritis: a systematic review and network meta-analysis
Abstract
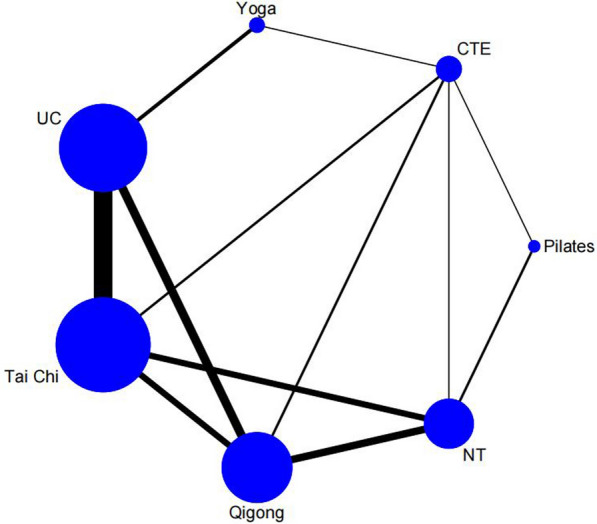
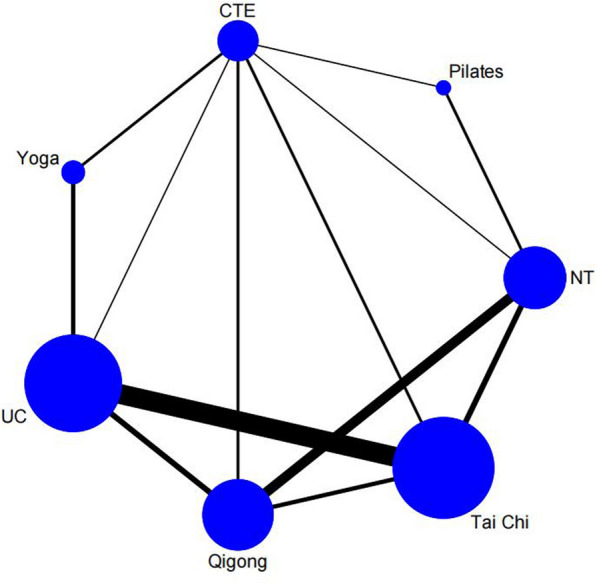
Introduction: Knee osteoarthritis (KOA) is a prevalent chronic joint disease. Due to the risks of opioid use and limited pharmacological effectiveness, mind-body exercise (MBE) therapy and other non-pharmacological interventions have emerged as first-line treatments for this condition. However, the optimal MBE modes for KOA remain undetermined. This systematic review and network meta-analysis (NMA) aims to compare the efficacy of different MBE modes, including Pilates, Tai Chi, Yoga, and Qigong, in managing KOA.
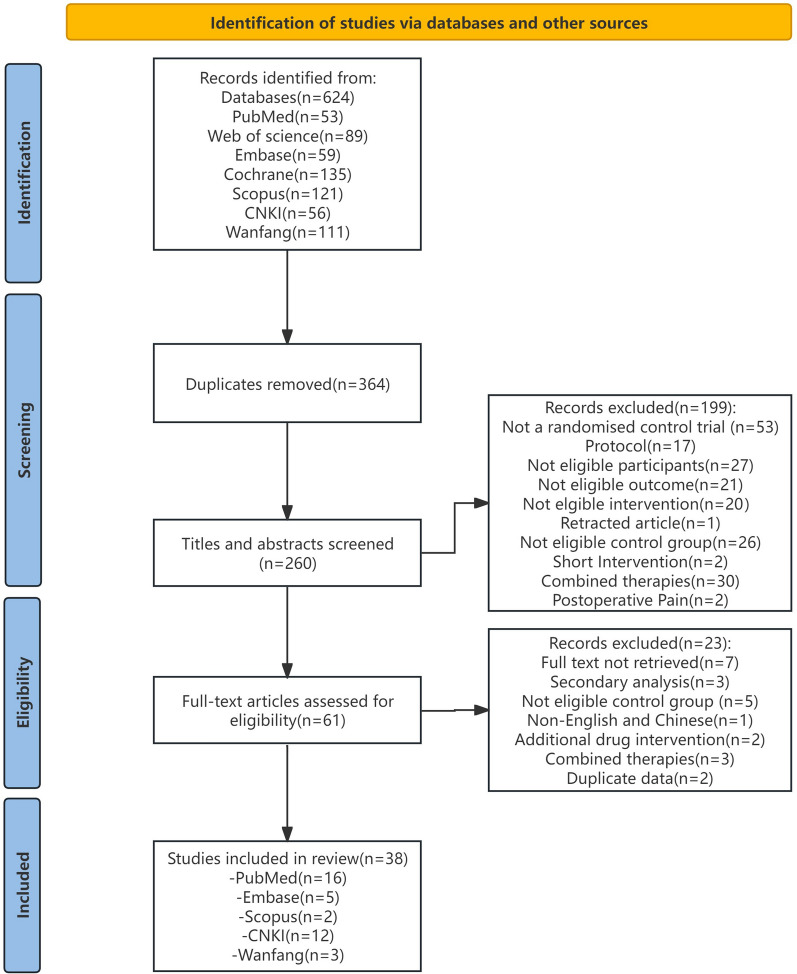
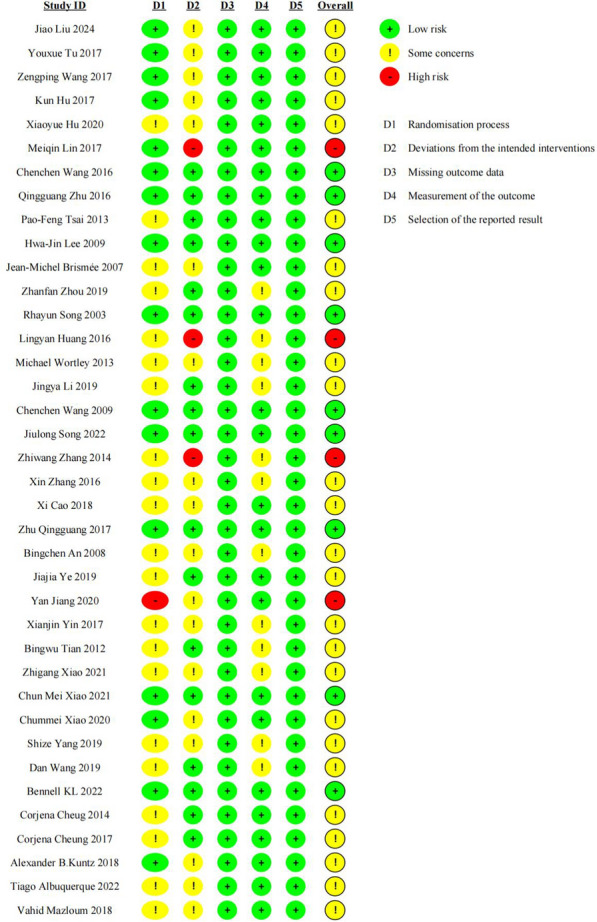
Methods: We searched PubMed, Embase, Cochrane Library, Web of Science, Scopus, China National Knowledge Infrastructure (CNKI), Wanfang Database from inception to 25 April 2024. Randomized clinical trials comparing MBE interventions for pain, physical function and quality of life (QoL) in KOA patients were eligible. The Cochrane Risk-of-Bias Tool 2.0 and Grading of Recommendations, Assessment, Development & Evaluation (GRADE) approach were used to assess literature quality and evidence certainty for each outcome.
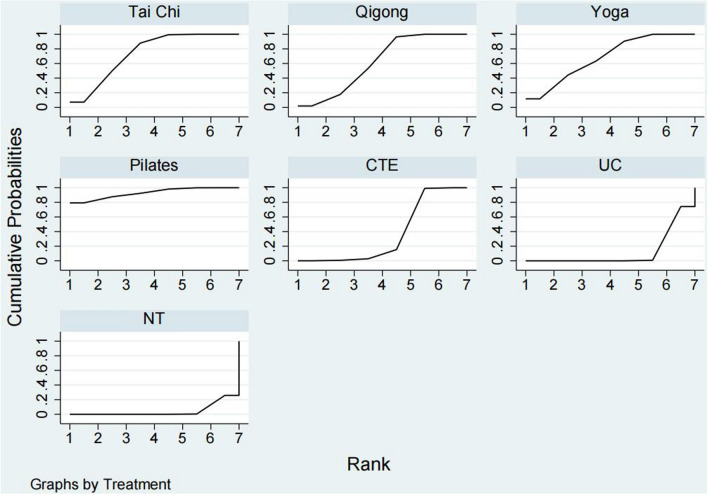
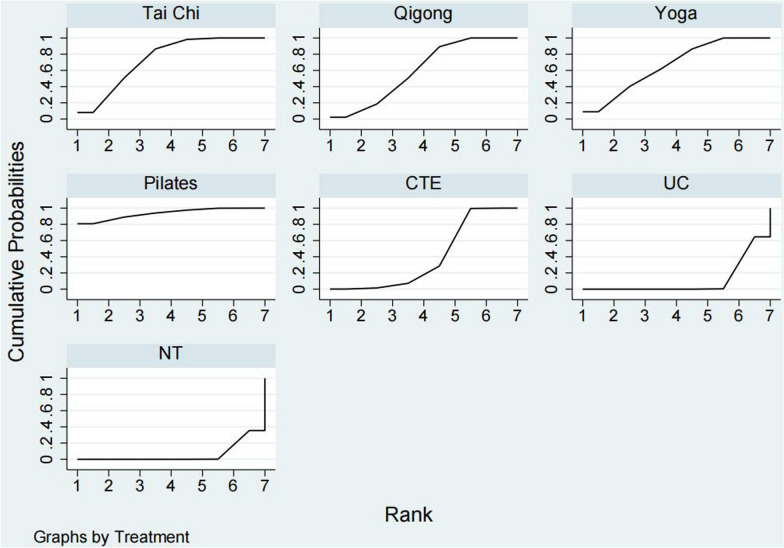
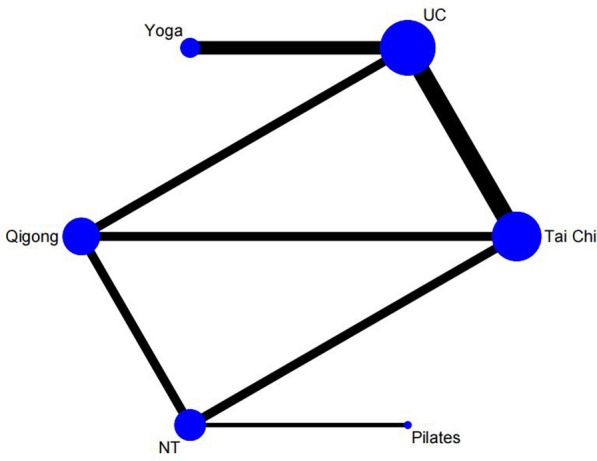
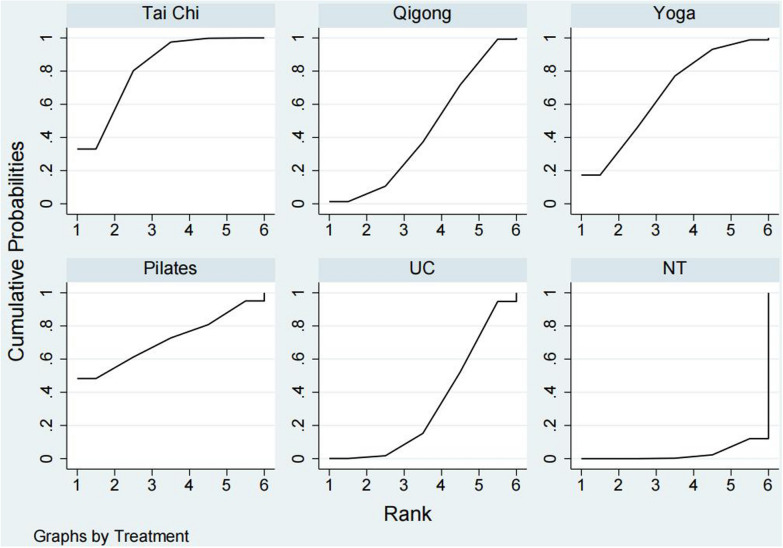
Result: A total of 38 studies (N = 2561) were included, with 38 for pain, 36 for physical function, and 12 for QoL in the NMA. With moderate-certainty, both Pilates and TC showed significant improvements in pain reduction [Pilates: standardized mean difference (SMD) = - 1.19, 95% confidence intervals (95% CI): - 1.92 to - 0.46; TC: SMD = - 0.78, 95% CI - 0.97 to - 0.59] and physical function (Pilates: SMD = - 1.37, 95% CI - 2.13 to - 0.50; TC: SMD = - 0.85, 95% CI - 1.08 to - 0.63) compared to the usual care group, while TC [SMD = - 0.57, 95% CI = (- 1.07 to - 0.06)] showed statistically significant efficacy in improving QoL compared to the usual care group.
Conclusion: There is moderate-certainty evidence that Pilates and Tai Chi may be the most effective mind-body exercises for improving pain and physical function in knee osteoarthritis, while Tai Chi may be the best for improving quality of life. These findings may help clinicians guide their prescription of exercise types with respect to treatment outcomes. The limited number of large sample studies and the few studies with low bias risk are limitations. Trial registration The protocol for NMA has been registered with PROSPERO (CRD42024531878).
Keywords: Knee osteoarthritis; Mind–body exercises; Network meta-analysis; Systematic review.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: Not applicable. Consent for publication: Not applicable. Competing interests: The authors declare that they have no competing interests.
Figures
Similar articles
-
Effects of mind-body exercise on knee osteoarthritis: a systematic review and meta-analysis of randomized controlled trials.BMC Musculoskelet Disord. 2024 Mar 22;25(1):229. doi: 10.1186/s12891-024-07278-4. BMC Musculoskelet Disord. 2024. PMID: 38515124 Free PMC article.
-
Efficacy of aerobic exercises for knee osteoarthritis: a network meta analysis of randomized clinical trials.J Orthop Surg Res. 2025 Jun 2;20(1):557. doi: 10.1186/s13018-025-05973-z. J Orthop Surg Res. 2025. PMID: 40452037 Free PMC article.
-
Mind-body exercises for osteoarthritis: an overview of systematic reviews including 32 meta-analyses.Disabil Rehabil. 2024 May;46(9):1699-1707. doi: 10.1080/09638288.2023.2203951. Epub 2023 Apr 28. Disabil Rehabil. 2024. PMID: 37115606 Review.
-
Effectiveness of Traditional Chinese Exercise for Symptoms of Knee Osteoarthritis: A Systematic Review and Meta-Analysis of Randomized Controlled Trials.Int J Environ Res Public Health. 2020 Oct 27;17(21):7873. doi: 10.3390/ijerph17217873. Int J Environ Res Public Health. 2020. PMID: 33121082 Free PMC article.
-
Are Mind-Body Exercise Beneficial for Treating Pain, Function, and Quality of Life in Middle-Aged and Old People With Chronic Pain? A Systematic Review and Meta-Analysis.Front Aging Neurosci. 2022 Jun 21;14:921069. doi: 10.3389/fnagi.2022.921069. eCollection 2022. Front Aging Neurosci. 2022. PMID: 35800981 Free PMC article.
References
-
- Sharma L. Osteoarthritis of the knee. N Engl J Med. 2021;384(1):51–9. - PubMed
-
- Kolasinski SL, Neogi T, Hochberg MC, Oatis C, Guyatt G, Block J, Callahan L, Copenhaver C, Dodge C, Felson D, et al. 2019 American college of rheumatology/arthritis foundation guideline for the management of osteoarthritis of the hand, hip, and knee. Arthritis Care Res (Hoboken). 2020;72(2):149–62. - PMC - PubMed
-
- Mahmoudian A, Lohmander LS, Mobasheri A, Englund M, Luyten FP. Early-stage symptomatic osteoarthritis of the knee—time for action. Nat Rev Rheumatol. 2021;17(10):621–32. - PubMed
-
- Steinmetz JD, Culbreth GT, Haile LM, Rafferty Q, Lo J, Fukutaki KG, Cruz JA, Smith AE, Vollset SE, Brooks PM, Cross M. Global, regional, and national burden of osteoarthritis, 1990–2020 and projections to 2050: a systematic analysis for the Global Burden of Disease Study 2021. Lancet Rheumatol. 2023;5(9):e508–22. - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
