

Short- and mid-term outcomes after redo surgical valve replacement
- PMID: 40247382
- PMCID: PMC12007241
- DOI: 10.1186/s40001-025-02563-x
Short- and mid-term outcomes after redo surgical valve replacement
Abstract
Background: While previous studies have indicated comparable outcomes for redo surgical valve replacement (SVR) and primary SVR, there is limited information regarding the long-term follow-up of these patients. Providing prognostic data on redo SVR is crucial for enhancing decision-making and medical care, as well as for identifying low-risk subsets of patients eligible for redo SVR. This study aimed to evaluate the short- and mid-term outcomes of patients who underwent their first and second redo SVR of a previously replaced valve.
Methods: We included 118 consecutive patients with a history of first or second redo SVR. The participants had a mean age of 57.5 ± 14.4 years, with 71 (60%) being female. The median follow-up period was 69 months. Clinical, intraoperative, and laboratory data were analyzed to assess all-cause mortality, major adverse events (MAE), and a composite of prosthetic valve thrombosis, embolic events, and major hemorrhage (TEH), along with their predictors. Bayesian model averaging was used for statistical analysis.
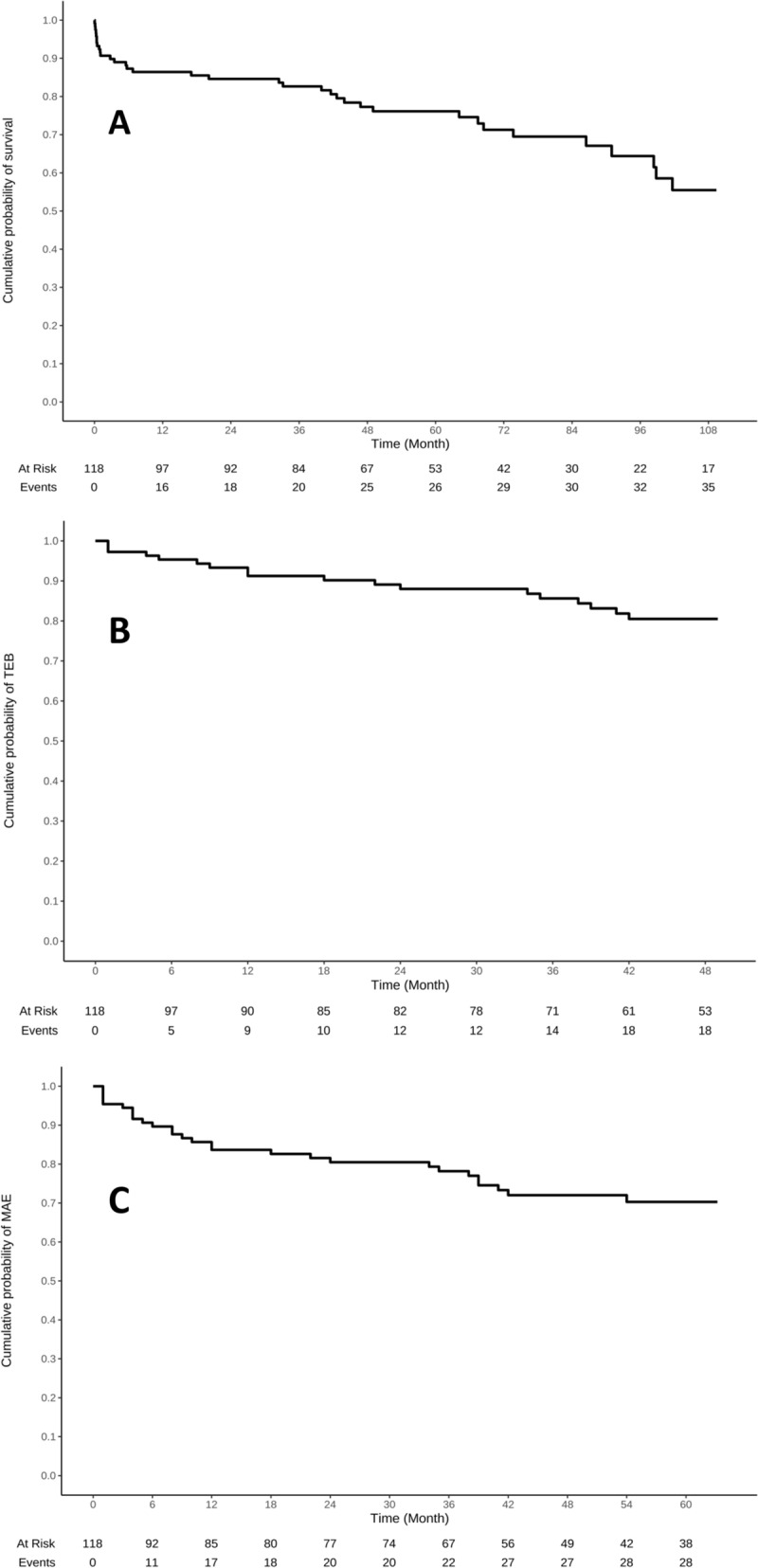
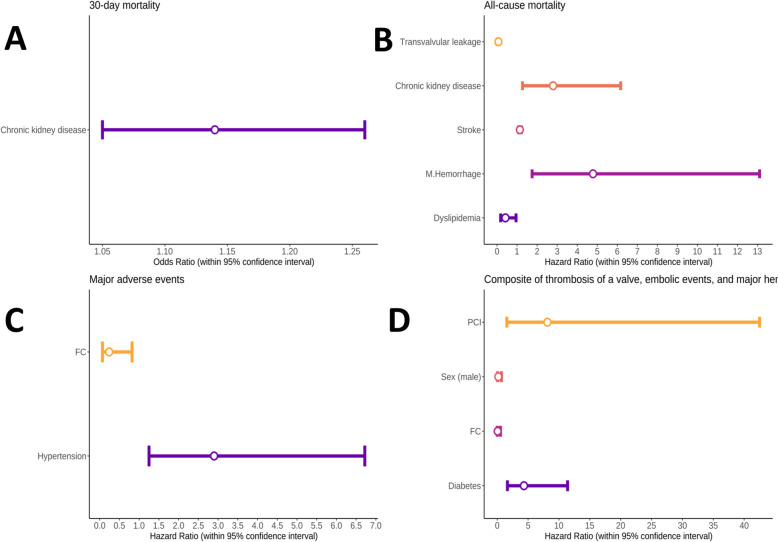
Results: The 30-day mortality rate was 11 patients (9.3%). Chronic kidney disease was identified as an independent predictor of 30-day mortality. The overall survival rates at one and five years were 86% (95% CI 80% to 93%) and 76% (95% CI 68% to 85%), respectively. Dyslipidemia, a history of major bleeding, chronic kidney disease, stroke, and transvalvular leakage in biological prostheses were all associated with all-cause mortality as independent predictors. The TEH-free survival rates at one and five years were 91% (95% CI 86% to 97%) and 79% (95% CI 71% to 88%), respectively. Diabetes, sex, a history of percutaneous coronary intervention, and baseline functional capacity were identified as independent predictors for the occurrence of TEH. The MAE-free survival rates at one and five years were 82% (95% CI 73% to 92%) and 61% (95% CI 49% to 75%), respectively. Hypertension and baseline functional class were independent predictors of MAE occurrence. The type and anatomical position of the valve were not predictors of mortality, THE, and MAE.
Conclusions: Our study demonstrated acceptable short- and mid-term outcomes for redo SVR, especially in patients without significant risk factors. Several potential predictors of adverse outcomes were identified.
Keywords: Mortality; Prognosis; Prosthetic valve; Redo surgery; Valve replacement.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: The research proposal was approved by the institutional review board (IR.TUMS.THC.REC.1401.005) following the 1964 Declaration of Helsinki and its later amendments. Written informed consent was obtained from the study population. Consent for publication: Not applicable. Competing interests: The authors declare no competing interests.
Figures
References
-
- Writing Committee Members, Otto CM, Nishimura RA, Bonow RO, Carabello BA, Erwin JP 3rd, Gentile F, Jneid H, Krieger EV, Mack M, McLeod C, O’Gara PT, Rigolin VH, Sundt TM 3rd, Thompson A, Toly C, ACC/AHA Joint Committee Members, O’Gara PT, Beckman JA, Levine GN, Al-Khatib SM, Armbruster A, Birtcher KK, Ciggaroa J, Deswal A, Dixon DL, Fleisher LA, de Las Fuentes L, Gentile F, Goldberger ZD, Gorenek B, Haynes N, Hernandez AF, Hlatky MA, Joglar JA, Jones WS, Marine JE, Mark D, Palaniappan L, Piano MR, Spatz ES, Tamis-Holland J, Wijeysundera DN, Woo YJ. ACC/AHA guideline for the management of patients with valvular heart disease: a report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. J Thorac Cardiovasc Surg. 2021;162(2):e183–353. 10.1016/j.jtcvs.2021.04.002. - DOI - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
