

Efficacy and safety of online adaptive magnetic resonance-guided fractionated stereotactic radiotherapy for brain metastases in non-small cell lung cancer (GASTO-1075): a single-arm, phase 2 trial
- PMID: 40247887
- PMCID: PMC12005306
- DOI: 10.1016/j.eclinm.2025.103189
Efficacy and safety of online adaptive magnetic resonance-guided fractionated stereotactic radiotherapy for brain metastases in non-small cell lung cancer (GASTO-1075): a single-arm, phase 2 trial
Abstract
Background: Brain metastases (BMs) in non-small cell lung cancer (NSCLC) are associated with poor prognosis and quality of life (QoL). This study aimed to evaluate the efficacy and safety of online adaptive MR-guided fractionated stereotactic radiotherapy (FSRT) using a 1.5 T MR-Linac in this subgroup of patients.
Methods: This single-arm phase 2 trial was conducted at Sun Yat-sen University Cancer Centre. Patients aged 18-75 years with NSCLC, 1-10 BMs, and an ECOG status of 0-1 were included. Key exclusion criteria included inability to undergo contrast-enhanced MRI and contraindications to bevacizumab. Patients received 30 Gy adaptive FSRT in 5 daily fractions under real-time MR guidance, with bevacizumab before (day 1) and after (day 21) FSRT. The primary endpoint was 1-year intracranial progression-free survival (IPFS); secondary endpoints included objective response rate (ORR), 1-year progression-free survival (PFS), 1-year overall survival (OS), treatment-related toxicities, and QoL. All enrolled patients were included in primary and safety analyses. This trial is registered with Clinicaltrials.gov, NCT04946019.
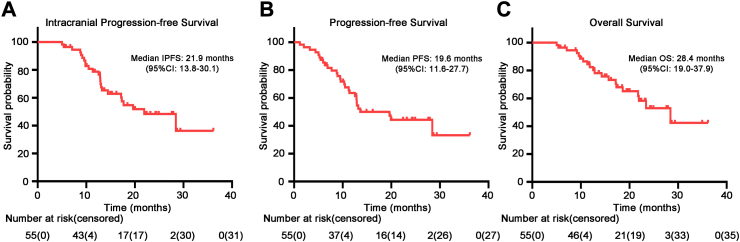
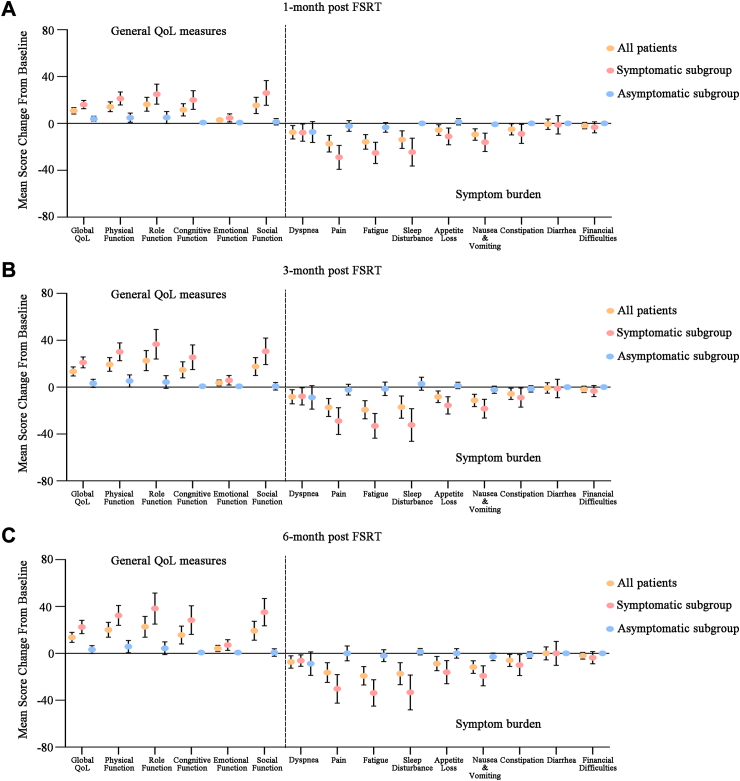
Findings: Between June 10th, 2021 and June 29th, 2023, 70 patients were assessed for eligibility and 55 patients were enrolled (median follow-up: 22.3 months). The median age was 58 years (IQR: 51-65), with 33% (18/55) female patients, and 82% (45/55) presenting with adenocarcinoma. The 1-year IPFS rate was 78.7% (95% CI, 68.2%-90.7%), with a median IPFS of 21.9 months (95% CI, 13.8-30.1 months). The 1-year PFS rate was 63.5% (95% CI: 51.8%-78.2%), and OS was 82.4% (95% CI: 72.6%-93.6%). The ORR reached 78% (95% CI: 65.0%-88.2%). Treatment-related toxicity was minimal, with only one case (2%) of grade 1 radiation necrosis. QoL improved steadily, with the Global Health Status score increasing from 65.67 ± 16.97 to 79.33 ± 8.79 at 6 months post FSRT (p < 0.0001).
Interpretation: Online adaptive FSRT using a 1.5 T MR-Linac has demonstrated effectiveness and good tolerability for BMs in patients with NSCLC. However, the relatively small sample size and short follow-up may affect result generalizability. Further randomised studies are warranted to confirm these findings and establish optimal treatment protocols.
Funding: The National Natural Science Foundation of China (Grant Number 82073328).
Keywords: Adaptive radiotherapy; Brain metastases; Fractionated stereotactic radiotherapy; MR-Linac; NSCLC.
© 2025 The Authors.
Conflict of interest statement
The authors declare no potential conflicts of interest.
Figures




Similar articles
-
Analysis of linear accelerator-based fractionated stereotactic radiotherapy in brain metastases: efficacy, safety, and dose tolerances.Front Oncol. 2024 Nov 21;14:1471004. doi: 10.3389/fonc.2024.1471004. eCollection 2024. Front Oncol. 2024. PMID: 39687885 Free PMC article.
-
Evaluating contouring accuracy and dosimetry impact of current MRI-guided adaptive radiation therapy for brain metastases: a retrospective study.J Neurooncol. 2024 Mar;167(1):123-132. doi: 10.1007/s11060-024-04583-9. Epub 2024 Feb 1. J Neurooncol. 2024. PMID: 38300388 Free PMC article.
-
An exploratory analysis of MR-guided fractionated stereotactic radiotherapy in patients with brain metastases.Clin Transl Radiat Oncol. 2023 Feb 23;40:100602. doi: 10.1016/j.ctro.2023.100602. eCollection 2023 May. Clin Transl Radiat Oncol. 2023. PMID: 36910023 Free PMC article.
-
Feasibility of linac-based fractionated stereotactic radiotherapy and stereotactic radiosurgery for patients with up to ten brain metastases.Radiat Oncol. 2022 Dec 28;17(1):213. doi: 10.1186/s13014-022-02185-1. Radiat Oncol. 2022. PMID: 36578021 Free PMC article.
-
Stereotactic radiosurgery versus stereotactic radiotherapy in the management of intracranial meningiomas: a systematic review and meta-analysis.Neurosurg Focus. 2019 Jun 1;46(6):E2. doi: 10.3171/2019.3.FOCUS1970. Neurosurg Focus. 2019. PMID: 31153149
References
-
- Sher T., Dy G.K., Adjei A.A. Small cell lung cancer. Mayo Clin Proc. 2008;83:355–367. - PubMed
-
- Andratschke N., Kraft J., Nieder C., et al. Optimal management of brain metastases in oncogenic-driven non-small cell lung cancer (NSCLC) Lung Cancer. 2019;129:63–71. - PubMed
-
- Bovi J.A., Pugh S.L., Sabsevitz D., et al. Pretreatment volume of MRI-determined white matter injury predicts neurocognitive decline after hippocampal avoidant whole-brain radiation therapy for brain metastases: secondary analysis of NRG Oncology radiation therapy oncology group 0933. Adv Radiat Oncol. 2019;4:579–586. - PMC - PubMed
Associated data
LinkOut - more resources
Full Text Sources
Medical
