

Effectiveness of a systematic home-based albuminuria screening programme to detect chronic kidney disease in high-risk individuals in primary care (SALINE): a cross-sectional screening study
- PMID: 40247889
- PMCID: PMC12005226
- DOI: 10.1016/j.eclinm.2025.103185
Effectiveness of a systematic home-based albuminuria screening programme to detect chronic kidney disease in high-risk individuals in primary care (SALINE): a cross-sectional screening study
Abstract
Background: Although guidelines recommend opportunistic screening for chronic kidney disease (CKD) in individuals with established risk factors, such as diabetes, hypertension, or cardiovascular disease, screening for CKD in these individuals remains suboptimal. This study aimed to evaluate the effectiveness of a systematic home-based albuminuria screening program in primary care patients at risk for CKD.
Methods: A cross-sectional screening study was performed in ten general practices and five pharmacies in the Netherlands from November 2021 to May 2024. A random selection of patients aged 45-80 years at risk for CKD based on risk factors registered in their electronic medical record was invited for home-based albuminuria screening using a urine collection device for measurement of the urinary albumin-to-creatinine ratio (ACR). In those patients with confirmed increased albuminuria (ACR ≥3 mg/mmol), an elaborate screening to assess the presence of CKD and cardiovascular risk factors was performed, followed by a referral to their general practitioner (GP) for evaluation of the findings. The primary outcome was the yield of the home-based albuminuria screening and elaborate screening to detect increased albuminuria in the GP and the pharmacy setting. SALINE is registered with ClinicalTrials.gov, NCT05321095.
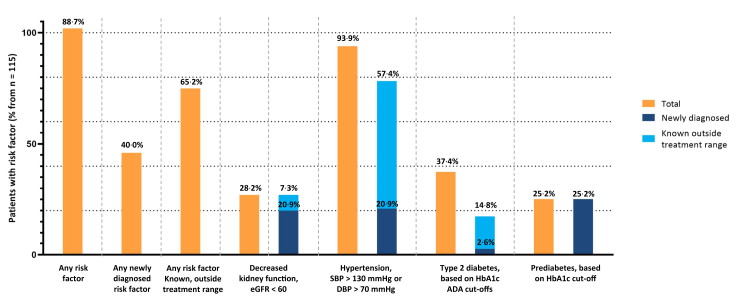
Findings: In total, 6380 patients (3802 via ten GPs and 2578 via five pharmacies) were invited for home-based albuminuria screening. The participation rate was 40·1% among patients invited via their GP (1524/3802), compared to 21·8% (562/2578) among those invited via their pharmacy (P < 0·001). In total, 8·7% of the GP participants had confirmed increased albuminuria (133/1524), compared to 6·0% of the pharmacy participants (34/562). Of the 115 GP participants with detected increased albuminuria who completed the elaborate screening, 102 (88·7%) were identified with one or more newly diagnosed CKD or cardiovascular risk factor(s) (n = 46, 40·0%), or with a known risk factor that was outside the target range for treatment (n = 75, 65·2%). Of the pharmacy participants with detected increased albuminuria completing the home-based screening, 26 completed the elaborate screening. Of those, 22 (84·6%) were identified with one or more newly diagnosed CKD or cardiovascular risk factor(s) (n = 6, 2·3%), or with a known risk factor that was outside the target range for treatment (n = 21, 80·8%).
Interpretation: Systematic albuminuria screening of patients at risk for CKD in primary care, when performed in addition to regular opportunistic screening, has an acceptable participation rate and yield when performed via GPs, whereas it is less effective when performed via pharmacies. Such a screening program identifies patients with yet unknown albuminuria who may benefit from starting or optimizing kidney and cardioprotective treatment. The introduction of such systematic albuminuria screening programs via GPs merits further study to optimize the participation and yield.
Funding: This study is funded by AstraZeneca Netherlands.
Keywords: Albuminuria; Chronic kidney disease; Primary care; Screening.
© 2025 The Author(s).
Conflict of interest statement
Professor Kocks reports grants, personal fees and non-financial support from AstraZeneca, grants, personal fees and non-financial support from Boehringer Ingelheim, grants and personal fees from Chiesi Pharmaceuticals, grants, personal fees and non-financial support from GSK, grants and personal fees from Novartis, grants from MundiPharma, grants from TEVA, outside the submitted work. He is the owner of GPRI and has stock options for 3% in Lothar MedTec. In the past three years, HJLH has received fees for consultancy or grants, or both, for research from AstraZeneca, Bayer, Boehringer Ingelheim, Chinook, CLS Pharma, Dimerix, Eli-Lilly, Fresenius, Gilead, Janssen, Novo Nordisk, and Travere Therapeutics. In the past three years, RTG has received fees for consultancy or grants, or both, for research from AbbVie, AstraZeneca, Baxter, Bayer, Healthy.io, Roche, and Sandoz. The other authors don't report any conflict of interest.
Figures

References
-
- Visseren F.L.J., Mach F., Smulders Y.M., et al. 2021 ESC Guidelines on cardiovascular disease prevention in clinical practice: developed by the Task Force for cardiovascular disease prevention in clinical practice with representatives of the European Society of Cardiology and 12 medical societies with the special contribution of the European Association of Preventive Cardiology (EAPC) Eur Heart J. 2021;42(34):3227–3337. doi: 10.1093/eurheartj/ehab484. - DOI - PubMed
Associated data
LinkOut - more resources
Full Text Sources
Medical
