

Medial patellofemoral ligament fixation with suture tape augmentation decreases lateral patellar motion without changing contact pressure
- PMID: 40248041
- PMCID: PMC12003563
- DOI: 10.1002/jeo2.70240
Medial patellofemoral ligament fixation with suture tape augmentation decreases lateral patellar motion without changing contact pressure
Abstract
Purpose: Medial patellofemoral ligament (MPFL) reconstruction has been the standard of care for recurrent patellar dislocations and chronic patellar instability. MPFL repair has been used as an alternative surgical option. The purpose of this study was to assess patellar stability and patellofemoral contact mechanics following MPFL fixation with suture tape augmentation. We hypothesized that lateral patellar motion would be reduced.
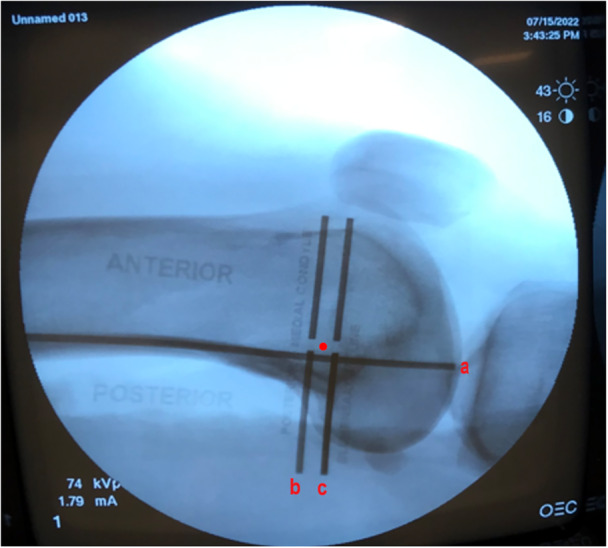
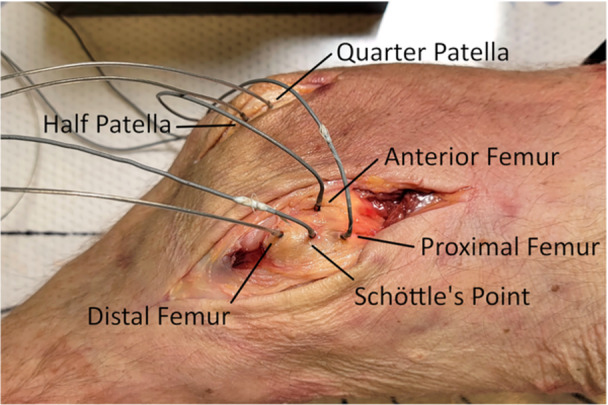
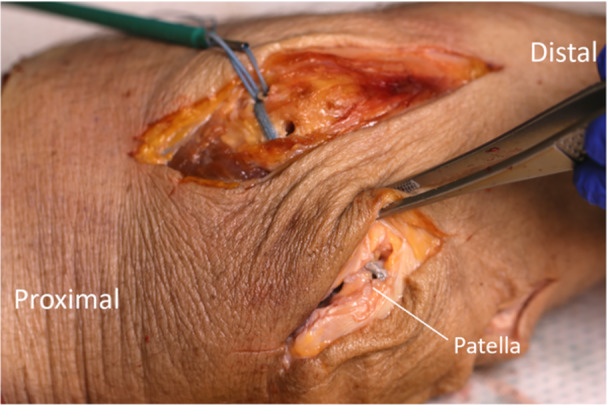
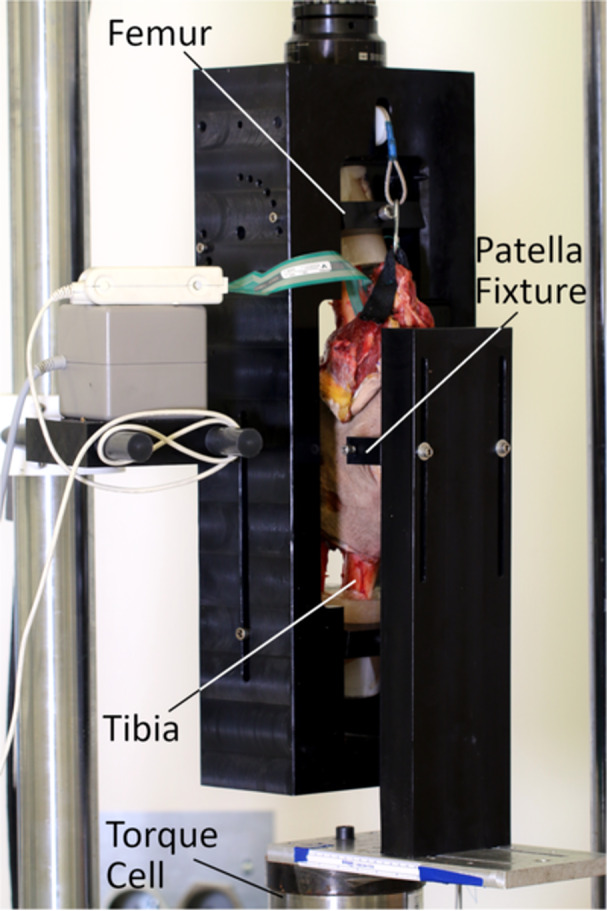
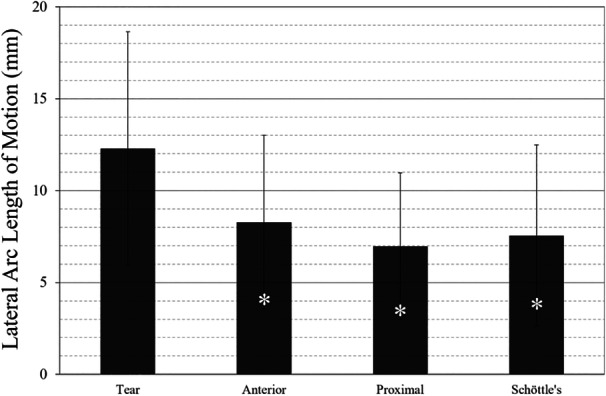
Methods: In twelve cadaver knees, a hole was drilled near the midpoint of the medial patella. Three locations were drilled on the femur Schöttle's point, 1 cm anterior to Schöttle's point and 1 cm proximal to Schöttle's point. Each knee was then held at 30° of knee flexion, and the patella was subjected to a physiologic lateral force. The resulting motion was measured, and patellofemoral contact forces were recorded. This process was performed with the MPFL torn and then bolstered with suture tape augmentation anchored centrally in the medial patella and each of the three femur hole locations.
Results: All MPFL augmentations provided significantly less lateral patellar motion compared to the torn condition. Contact area was significantly greater in the augmented condition than in the torn condition, but no statistical differences were observed in patellofemoral contact pressure. No significant differences in lateral patellar motion, contact pressure or contact area were found between femoral anchor positions.
Conclusions: MPFL fixation with suture tape augmentation significantly decreased lateral patellar motion compared to the torn condition without causing significant changes in contact pressures within the patellofemoral joint.
Level of evidence: N/A.
Keywords: MPFL augmentation; Schöttle's point; biomechanics.
© 2025 The Author(s). Journal of Experimental Orthopaedics published by John Wiley & Sons Ltd on behalf of European Society of Sports Traumatology, Knee Surgery and Arthroscopy.
Conflict of interest statement
Dr. Nima Rezaie declares that educational support is available from Arthrex (the study sponsor), Fones Marketing Management and Smith & Nephew. Dr. Wesley R. Stroud declares educational support from Prime Surgical and Smith & Nephew and reimbursement for travel and lodging from Zimmer Biomet. Dr. Jeffrey R. Dugas is/was a paid consultant for Arthrex (the study sponsor), Bioventus, DJO and Royal Biologics. Dr. Jeffrey R. Dugas has received non‐consulting and/or speaking fees, reimbursement for travel and lodging, and royalties/licences for Arthrex (the study sponsor). Dr. Jeffrey R. Dugas declares educational support, hospitality and royalties/licences from DJO. The remaining authors declare no conflicts of interest.
Figures
References
-
- Amis AA, Firer P, Mountney J, Senavongse W, Thomas NP. Anatomy and biomechanics of the medial patellofemoral ligament. Knee. 2003;10(3):215–220. - PubMed
-
- Arthrex . Medial patellofemoral ligament (MPFL) reconstruction surgical technique. 2021.
-
- Bicos J, Fulkerson JP, Amis A. Current concepts review: the medial patellofemoral ligament. Am J Sports Med. 2007;35(3):484–492. - PubMed
-
- Black SR, Meyers KN, Nguyen JT, Green DW, Brady JM, Maher SA, et al. Comparison of ligament isometry and patellofemoral contact pressures for medial patellofemoral ligament reconstruction techniques in skeletally immature patients. Am J Sports Med. 2020;48(14):3557–3565. - PubMed
LinkOut - more resources
Full Text Sources
Medical
Research Materials
