

Association of the non-high-density lipoprotein cholesterol to high-density lipoprotein cholesterol ratio (NHHR) with COPD prevalence and all-cause mortality: a population-based study based on NHANES 2007-2016
- PMID: 40248071
- PMCID: PMC12003284
- DOI: 10.3389/fmed.2025.1533744
Association of the non-high-density lipoprotein cholesterol to high-density lipoprotein cholesterol ratio (NHHR) with COPD prevalence and all-cause mortality: a population-based study based on NHANES 2007-2016
Abstract
Background: The non-high-density lipoprotein cholesterol to high-density lipoprotein cholesterol ratio (NHHR) plays a potential role in metabolic and cardiovascular diseases. However, its association with chronic obstructive pulmonary disease (COPD) is not well-defined. Here, we aim to investigate the potential association of NHHR with both the prevalence of COPD and all-cause mortality among individuals with COPD.
Methods: This population-based NHANES (2007-2016) study utilized weighted statistical analyses. Multivariable logistic regression assessed the NHHR-COPD prevalence association, with restricted cubic spline (RCS) testing for non-linearity. The association between NHHR and all-cause mortality in COPD was evaluated using Cox proportional hazards models and Kaplan-Meier, with RCS testing for non-linearity. Subgroup and sensitivity analyses confirmed the findings' reliability.
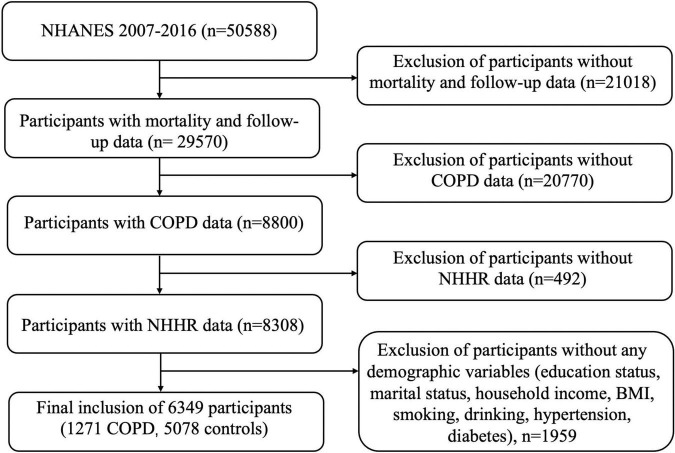
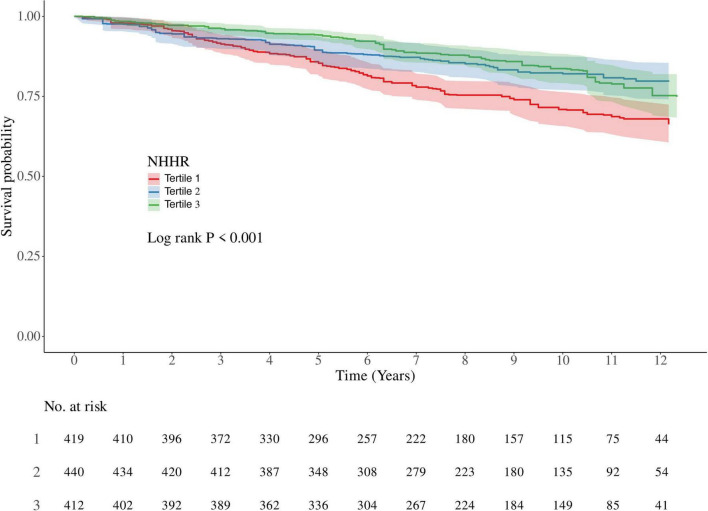
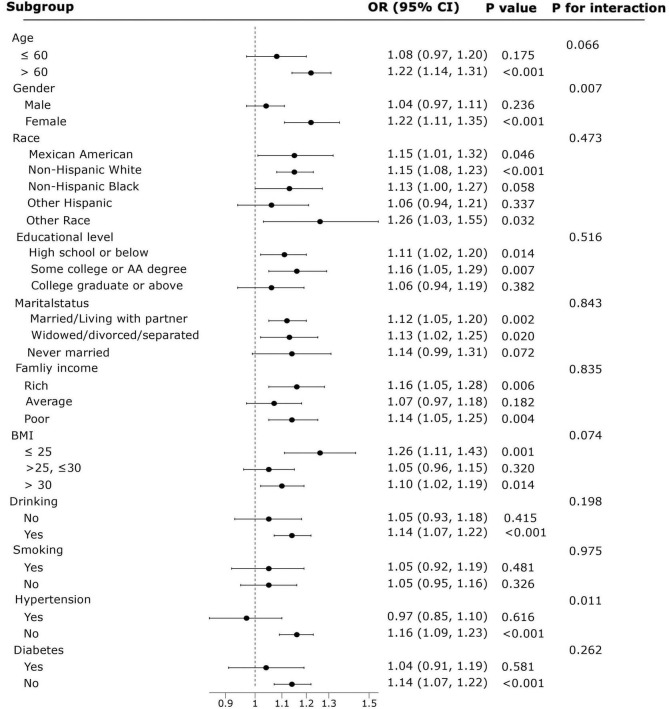
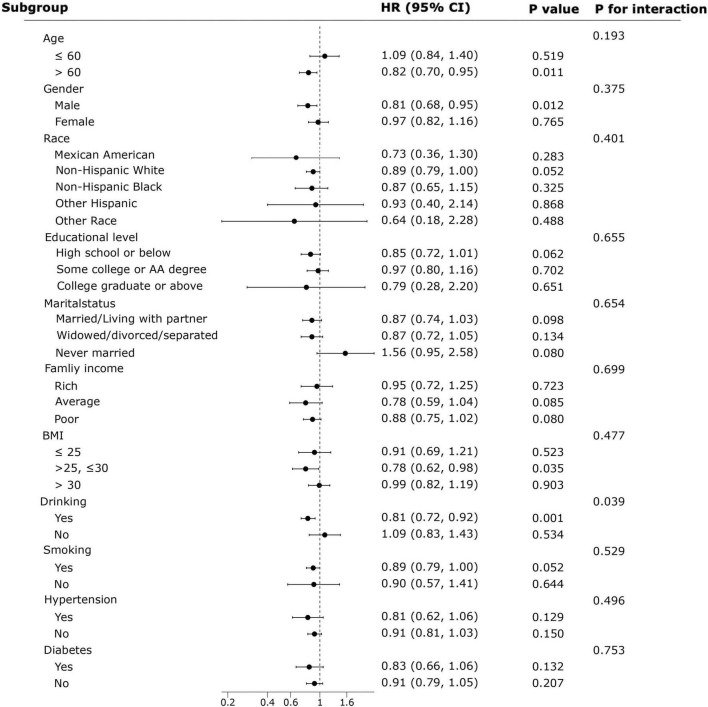
Results: This study included 6349 participants, of whom 1271 were diagnosed with COPD. Participants in the highest NHHR tertile demonstrated 62% higher odds of COPD prevalence compared to those in the lowest tertile (OR = 1.62, 95% CI:1.11-2.39, P = 0.017). Results from RCS analysis indicated a nonlinear relationship between NHHR and the prevalence of COPD (P for nonlinear = 0.007), with the curve demonstrating an inverted L-shape. Over an average follow-up period of 93 months, 320 participants with COPD died. In the weighted Kaplan-Meier survival analysis, participants with COPD in the lower NHHR tertile demonstrated greater cumulative probability of all-cause mortality compared to higher tertiles (P < 0.001). Weighted multivariable Cox regression models revealed an inverse association between NHHR levels and COPD all-cause mortality, with the highest NHHR tertile showing 11% lower likelihood of COPD all-cause mortality relative to the lowest tertile (HR = 0.89, 95% CI:0.80-0.99, P = 0.027). In addition, RCS analysis demonstrated a significant negative linear association between NHHR levels and all-cause mortality in COPD patients (P for nonlinear = 0.081). Subgroup and sensitivity analyses further confirmed the associations of NHHR on both morbidity and all-cause mortality.
Conclusion: Higher NHHR levels were associated with increased COPD prevalence yet inversely correlated with all-cause mortality in COPD patients. These paradoxical associations underscore the need for COPD-specific lipid management strategies that balance disease progression and mortality risks.
Keywords: COPD prevalence; NHANES; NHHR; all-cause mortality; lipid.
Copyright © 2025 Liu, Fan, Ren and Zheng.
Conflict of interest statement
The authors declare that the research was conducted without any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures

References
-
- Lozano R, Naghavi M, Foreman K, Lim S, Shibuya K, Aboyans V, et al. Global and regional mortality from 235 causes of death for 20 age groups in 1990 and 2010: A systematic analysis for the Global Burden of disease study 2010. Lancet. (2012) 380:2095–128. 10.1016/S0140-6736(12)61728-0 - DOI - PMC - PubMed
-
- Vos T, Flaxman A, Naghavi M, Lozano R, Michaud C, Ezzati M, et al. Years lived with disability (YLDs) for 1160 sequelae of 289 diseases and injuries 1990-2010: A systematic analysis for the Global Burden of disease study 2010. Lancet. (2012) 380:2163–96. 10.1016/S0140-6736(12)61729-2 - DOI - PMC - PubMed
-
- Walters J, Cameron-Tucker H, Courtney-Pratt H, Nelson M, Robinson A, Scott J, et al. Supporting health behaviour change in chronic obstructive pulmonary disease with telephone health-mentoring: Insights from a qualitative study. BMC Fam Pract. (2012) 13:55. 10.1186/1471-2296-13-55 - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources