

A German multicenter real-world analysis of talquetamab in 138 patients with relapsed/refractory multiple myeloma
- PMID: 40248128
- PMCID: PMC12005056
- DOI: 10.1002/hem3.70114
A German multicenter real-world analysis of talquetamab in 138 patients with relapsed/refractory multiple myeloma
Abstract
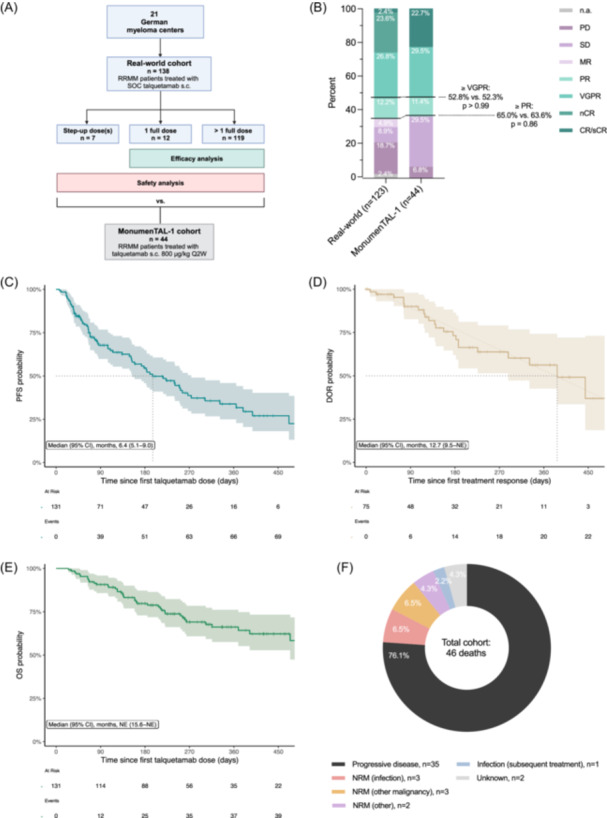
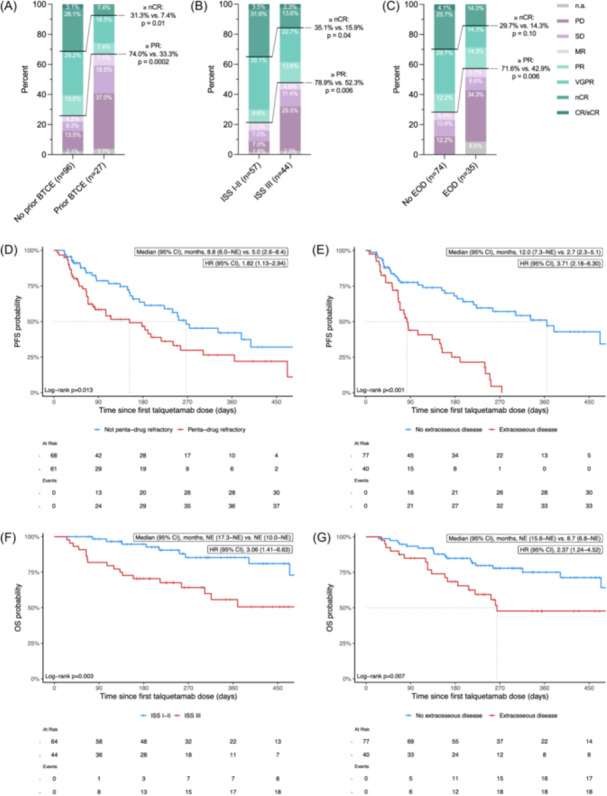
Bispecific T-cell engagers (BTCEs) represent a paradigm shift in the treatment of relapsed/refractory multiple myeloma (RRMM). Talquetamab, a GPRC5DxCD3 BTCE, has shown promising results in the MonumenTAL-1 trial and was recently approved by the Food and Drug Administration and the European Medicines Agency. However, treatment under real-world conditions may not represent patient characteristics in clinical trials with restricted enrollment criteria. We performed a retrospective real-world analysis including 138 RRMM patients treated with talquetamab at 21 German centers. Of evaluable patients, 43% had ISS stage III, 37% had extraosseous disease, and 48% had high-risk cytogenetics. After a median of six prior therapy lines, 58% of patients would not have been eligible for MonumenTAL-1. With a median follow-up of 8.2 months, we observed an overall response rate of 65% and a median progression-free survival of 6.4 months (95% confidence interval 5.1-9.0). Prior BTCE exposure, ISS stage III, extraosseous disease, and penta-drug refractory disease were associated with unfavorable outcomes. Grade ≥ 3 cytokine release syndrome and neurotoxicity occurred in 5.1% and 1.5% of patients, respectively. In summary, our real-world study confirms the efficacy and safety of talquetamab, despite a high proportion of patient- and disease-related risk factors. These results support its use as bridging or long-term treatment, even in advanced stages.
© 2025 The Author(s). HemaSphere published by John Wiley & Sons Ltd on behalf of European Hematology Association.
Conflict of interest statement
J. H. F. declares an advisory role for Pfizer and has received honoraria from BMS and Stemline and travel and congress participation grants from Janssen‐Cilag. C. R. has received honoraria from Janssen‐Cilag. F. Ba. has received honoraria and/or travel/accommodation expenses from BMS, AbbVie, and Janssen. B. B. has received honoraria from Janssen‐Cilag, GSK, Amgen, Sanofi, Takeda, Pfizer, and Oncopeptides. M. B. has received honoraria from Janssen, GSK, and AstraZeneca. A. B. has participated in advisory boards from BMS, Janssen, GSK, Sanofi, AstraZeneca, and Menarini; received honoraria from Menarini; and received honoraria and travel support from BMS, Janssen, GSK, Sanofi, AstraZeneca, Amgen, and Takeda. I. K. has received honoraria from AstraZeneca and educational/travel grants from Incyte, BeiGene, AstraZeneca, Janssen, and Pfizer. J. K. has received honoraria and/or travel/accommodation expenses from BMS, AbbVie, Sanofi, Pfizer, and Janssen. M. K. has received honoraria from GSK and Pfizer, and travel support from GSK, Janssen, Oncopeptides, Takeda, and Stemline. T. L. declares a consulting or advisory role for Janssen and has received research funding from Sanofi (to institution) and support for traveling, accommodations, and expenses from Sanofi, Lilly, Janssen, AOP Health, BeiGene, Alexion, and Regeneron. I. v. M. has participated in advisory boards and received honoraria from AbbVie, Janssen, BMS, GSK, Amgen, Sanofi, Pfizer, Oncopeptides, Stemline, and Takeda. C. S. M. declares a consulting or advisory role for BMS, Amgen, GSK, Janssen, and Sanofi, and has received honoraria and/or travel support from BMS, Amgen, GSK, Janssen, Sanofi, and Pfizer. S. T. has received honoraria from Janssen, Sanofi, Pfizer, Amgen, AbbVie, BMS, Menarini, Stemline, GSK, Takeda, and Kyowa Kirin. K. T. G. has received consulting fees from Sanofi, Takeda, Novartis, Amgen, GSK, and Janssen and honoraria from Novartis, Amgen, and GSK. R. W. consulted for and/or received honoraria from AbbVie, Alexion, Amgen, BMS, Janssen, Kite/Gilead, Novartis, Pfizer, Sanofi, and Takeda, and received research funding from Janssen and Sanofi (all paid to UKF). M. Hä. has received honoraria from SOBI, Novartis, Gilead, Falk Foundation, BMS, and Kite, and declares a consulting role for Pfizer, Incyte, Sanofi, Roche, Amgen, SOBI, Janssen, Kite, BMS, and BeiGene. L. R. declares a consulting or advisory role for BMS, Amgen, GSK, Janssen, Sanofi, and Pfizer, and has received research funding from BMS, travel support from Janssen and BeiGene, and honoraria from BMS, Janssen, Pfizer, and Sanofi. M. S. R. declares a consulting or advisory role for BMS, Amgen, GSK, Janssen, Sanofi, Pfizer, AbbVie, and Takeda, and has received research funding from BMS, Janssen, Sanofi, and Heidelberg Pharma; travel support from BMS, Amgen, and Janssen; and honoraria from BMS, Janssen, AbbVie, and Sanofi. R. T., J. B., F. Br., M. D., R. F., D. N. G., S. G. M., C. H., M. Hö., C. K., K. K., V. L., M. M., C. M. T., and R. Z. declare no potential competing interests.
Figures
References
-
- Rodriguez‐Otero P, Usmani S, Cohen AD, et al. International Myeloma Working Group immunotherapy committee consensus guidelines and recommendations for optimal use of T‐cell‐engaging bispecific antibodies in multiple myeloma. Lancet Oncol. May 2024;25(5):e205–16. - PubMed
LinkOut - more resources
Full Text Sources