

High-throughput screening of FDA-approved drugs identifies colchicine as a potential therapeutic agent for atypical teratoid/rhabdoid tumors (AT/RTs)
- PMID: 40248220
- PMCID: PMC12004362
- DOI: 10.1039/d5ra01341k
High-throughput screening of FDA-approved drugs identifies colchicine as a potential therapeutic agent for atypical teratoid/rhabdoid tumors (AT/RTs)
Abstract
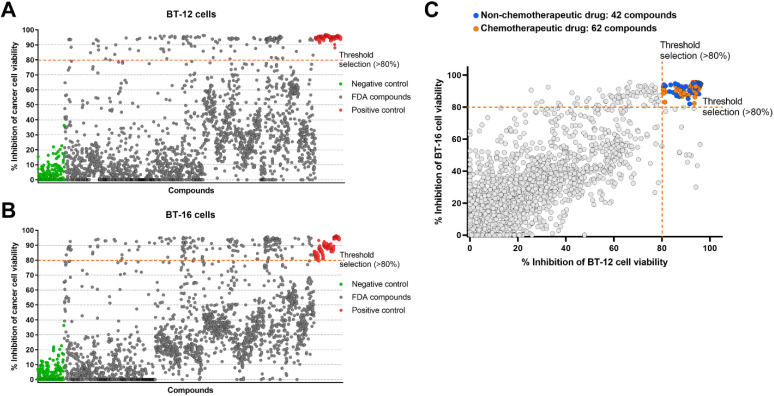
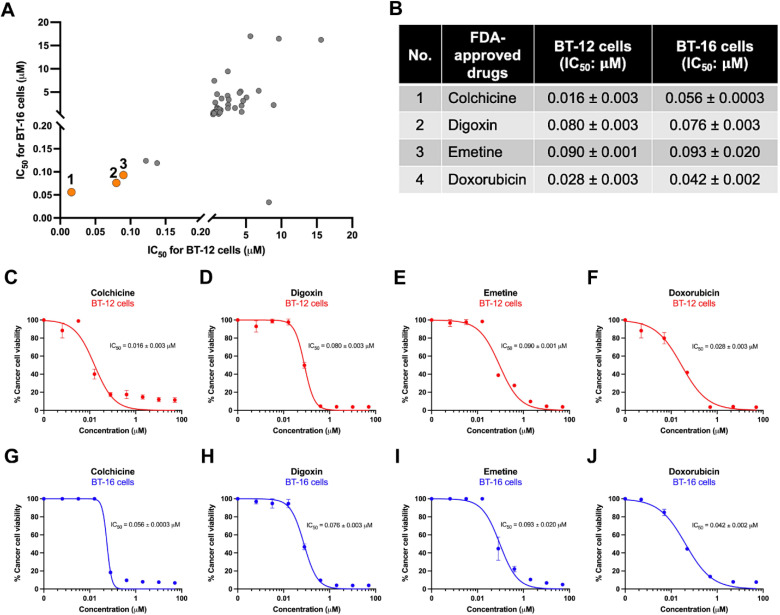
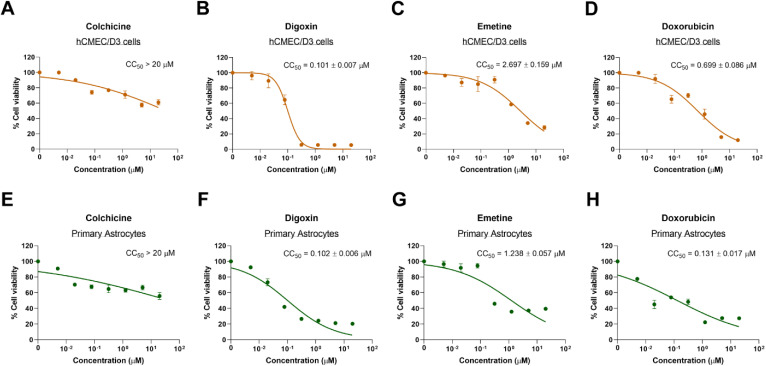
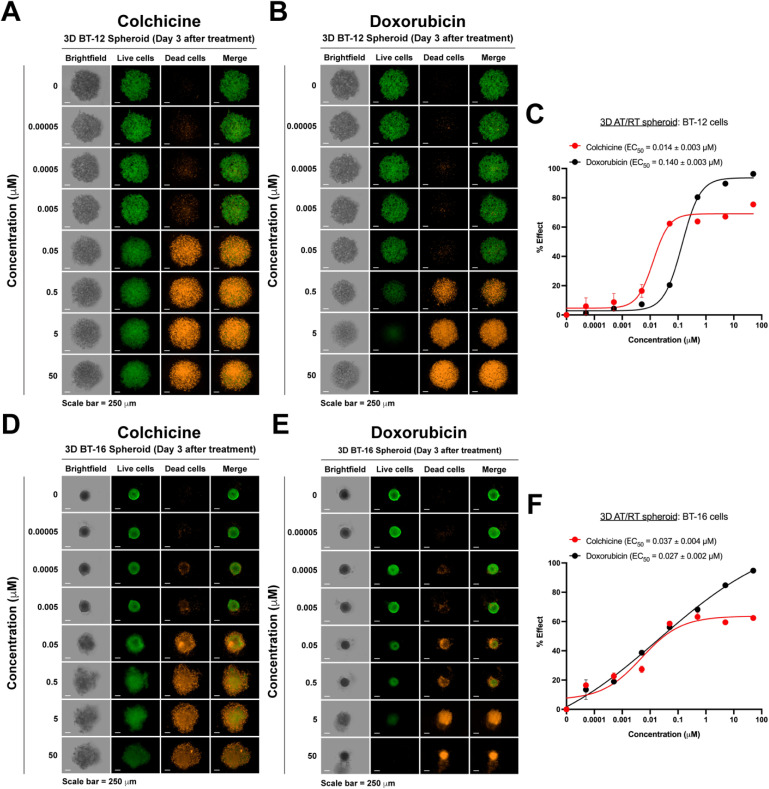
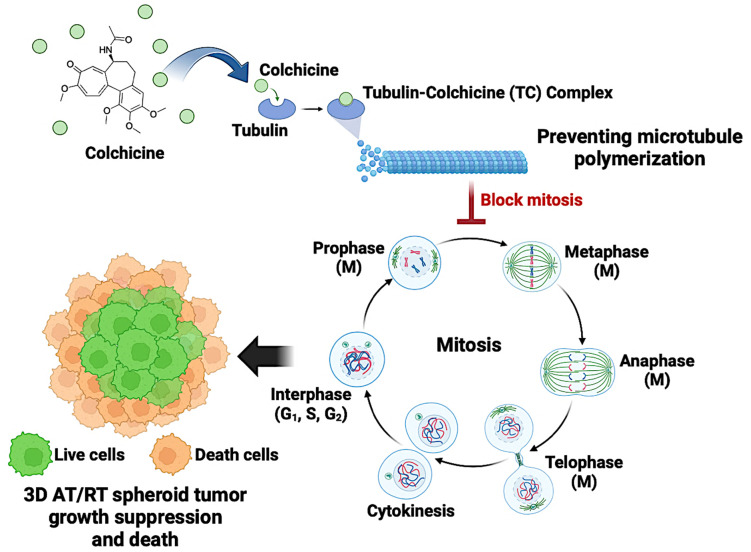
Atypical teratoid/rhabdoid tumor (AT/RT) is a rare and aggressive tumor of the primary central nervous system primarily affecting children. It typically originates in the cerebellum and brain stem and is associated with a low survival rate. While standard chemotherapy has been used as a primary treatment for AT/RTs, its success rate is unsatisfactory, and patients often experience severe side effects. Therefore, there is an urgent need to develop new and effective treatment strategies. One promising approach for identifying new therapies is drug repurposing. Although many FDA-approved drugs have been repurposed for various cancers, there have been no reports of such applications for AT/RTs. In this study, a library of 2130 FDA-approved drugs was screened using a high-throughput screening system against 2D traditional cultures and 3D spheroid cultures of AT/RT cell lines (BT-12 and BT-16). From this screening, colchicine, a non-chemotherapeutic agent, was identified as a promising candidate. It exhibited IC50 values of 0.016 and 0.056 μM against 2D BT-12 and 2D BT-16 cells, respectively, and IC50 values of 0.004 and 0.023 μM against 3D BT-12 and BT-16 spheroid cultures. Additionally, the cytotoxic effects of colchicine on human brain endothelial cells and human astrocytes were evaluated, and CC50 > 20 μM was observed, which is over two orders of magnitude higher than its effective concentrations in AT/RT cells, indicating considerably lower toxicity to normal brain cells and brain endothelial cells. In conclusion, colchicine shows significant potential to be repurposed as a treatment for AT/RTs, providing a safer and more effective therapeutic option for this rare and challenging disease.
This journal is © The Royal Society of Chemistry.
Conflict of interest statement
There are no conflicts to declare.
Figures
Similar articles
-
Identification of RPL5 and RPL10 as novel diagnostic biomarkers of Atypical teratoid/rhabdoid tumors.Cancer Cell Int. 2018 Nov 20;18:190. doi: 10.1186/s12935-018-0681-1. eCollection 2018. Cancer Cell Int. 2018. PMID: 30479569 Free PMC article.
-
Central nervous system atypical teratoid/rhabdoid tumors of infancy and childhood.Ultrastruct Pathol. 1997 Jul-Aug;21(4):369-78. doi: 10.3109/01913129709021935. Ultrastruct Pathol. 1997. PMID: 9206002 Review.
-
Primary intracranial atypical teratoid/rhabdoid tumors of infancy and childhood: MRI features and patient outcomes.AJNR Am J Neuroradiol. 2006 May;27(5):962-71. AJNR Am J Neuroradiol. 2006. PMID: 16687525 Free PMC article.
-
Rhabdoid tumors in patients conceived following ART: is there an association?Hum Reprod. 2023 Oct 3;38(10):2028-2038. doi: 10.1093/humrep/dead154. Hum Reprod. 2023. PMID: 37553222
-
Molecular targeted therapies for pediatric atypical teratoid/rhabdoid tumors.Pediatr Investig. 2022 May 23;6(2):111-122. doi: 10.1002/ped4.12325. eCollection 2022 Jun. Pediatr Investig. 2022. PMID: 35774526 Free PMC article. Review.
References
-
- Bhattacharjee M. Hicks J. Langford L. Dauser R. Strother D. Chintagumpala M. Horowitz M. Cooley L. Vogel H. Ultrastruct. Pathol. 1997;21:369–378. - PubMed
-
- Gökden N. Nappi O. Swanson P. E. Pfeifer J. D. Vollmer R. T. Wick M. R. Humphrey P. A. Am. J. Surg. Pathol. 2000;24:1329–1338. - PubMed
-
- Versteege I. Sévenet N. Lange J. Rousseau-Merck M.-F. Ambros P. Handgretinger R. Aurias A. Delattre O. Nature. 1998;394:203–206. - PubMed
-
- Louis D. N. Perry A. Reifenberger G. von Deimling A. Figarella-Branger D. Cavenee W. K. Ohgaki H. Wiestler O. D. Kleihues P. Ellison D. W. Acta Neuropathol. 2016;131:803–820. - PubMed
-
- Dho Y. S. Kim S. K. Cheon J. E. Park S. H. Wang K. C. Lee J. Y. Phi J. H. Childs Nerv. Syst. 2015;31:1305–1311. - PubMed
LinkOut - more resources
Full Text Sources