

Artificial Intelligence Models for Pediatric Lung Sound Analysis: Systematic Review and Meta-Analysis
- PMID: 40249944
- PMCID: PMC12048790
- DOI: 10.2196/66491
Artificial Intelligence Models for Pediatric Lung Sound Analysis: Systematic Review and Meta-Analysis
Abstract
Background: Pediatric respiratory diseases, including asthma and pneumonia, are major causes of morbidity and mortality in children. Auscultation of lung sounds is a key diagnostic tool but is prone to subjective variability. The integration of artificial intelligence (AI) and machine learning (ML) with electronic stethoscopes offers a promising approach for automated and objective lung sound.
Objective: This systematic review and meta-analysis assess the performance of ML models in pediatric lung sound analysis. The study evaluates the methodologies, model performance, and database characteristics while identifying limitations and future directions for clinical implementation.
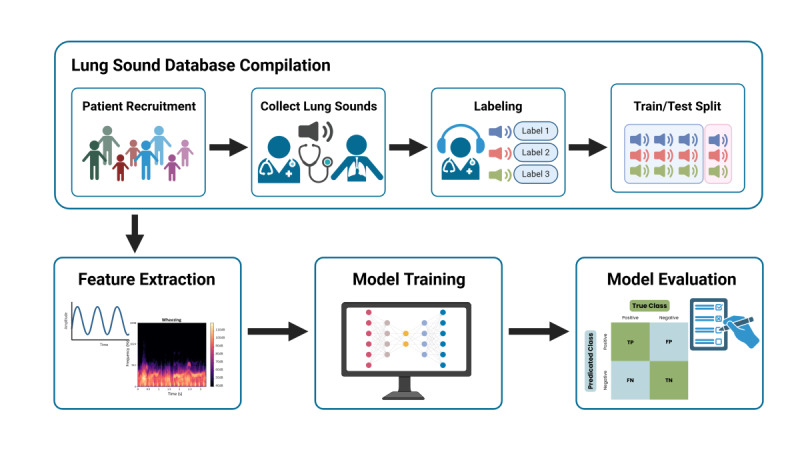
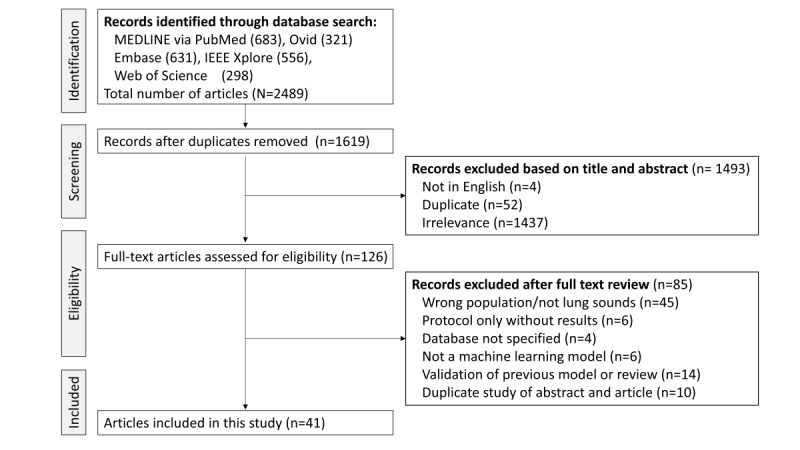
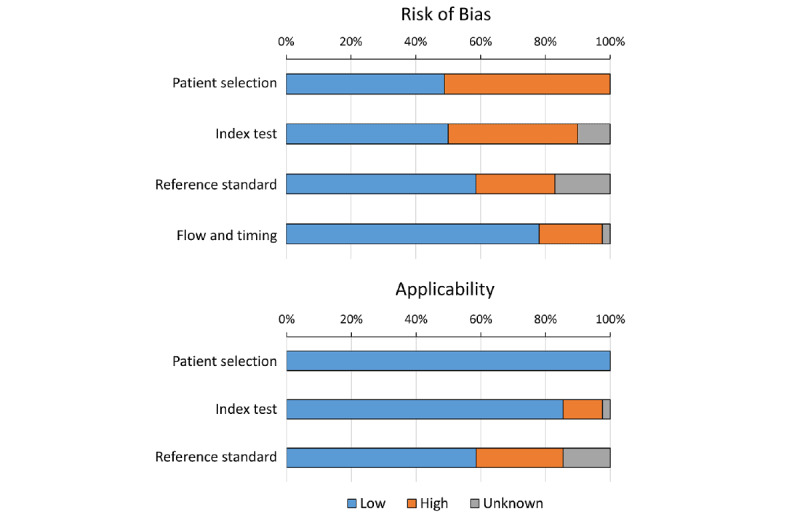
Methods: A systematic search was conducted in Medline via PubMed, Embase, Web of Science, OVID, and IEEE Xplore for studies published between January 1, 1990, and December 16, 2024. Inclusion criteria are as follows: studies developing ML models for pediatric lung sound classification with a defined database, physician-labeled reference standard, and reported performance metrics. Exclusion criteria are as follows: studies focusing on adults, cardiac auscultation, validation of existing models, or lacking performance metrics. Risk of bias was assessed using a modified Quality Assessment of Diagnostic Accuracy Studies (version 2) framework. Data were extracted on study design, dataset, ML methods, feature extraction, and classification tasks. Bivariate meta-analysis was performed for binary classification tasks, including wheezing and abnormal lung sound detection.
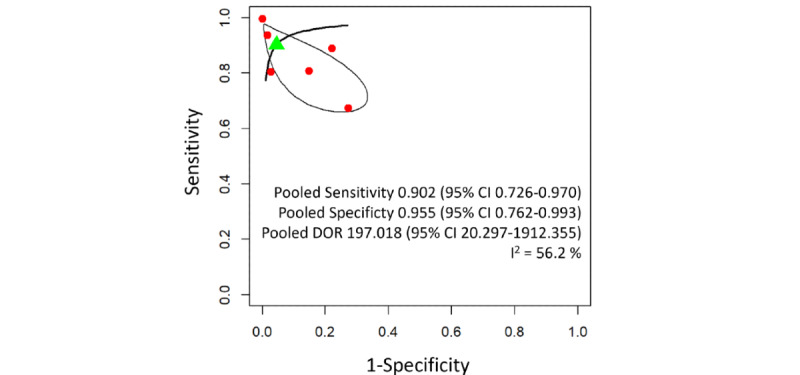
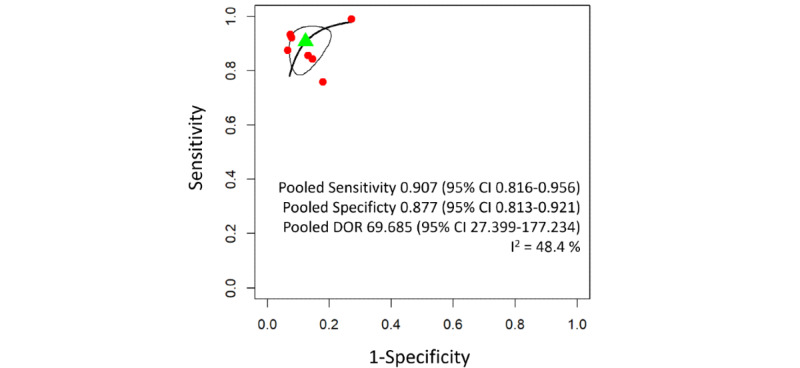
Results: A total of 41 studies met the inclusion criteria. The most common classification task was binary detection of abnormal lung sounds, particularly wheezing. Pooled sensitivity and specificity for wheeze detection were 0.902 (95% CI 0.726-0.970) and 0.955 (95% CI 0.762-0.993), respectively. For abnormal lung sound detection, pooled sensitivity was 0.907 (95% CI 0.816-0.956) and specificity 0.877 (95% CI 0.813-0.921). The most frequently used feature extraction methods were Mel-spectrogram, Mel-frequency cepstral coefficients, and short-time Fourier transform. Convolutional neural networks were the predominant ML model, often combined with recurrent neural networks or residual network architectures. However, high heterogeneity in dataset size, annotation methods, and evaluation criteria were observed. Most studies relied on small, single-center datasets, limiting generalizability.
Conclusions: ML models show high accuracy in pediatric lung sound analysis, but face limitations due to dataset heterogeneity, lack of standard guidelines, and limited external validation. Future research should focus on standardized protocols and the development of large-scale, multicenter datasets to improve model robustness and clinical implementation.
Keywords: abnormal lung sound detection; artificial intelligence; asthma; auscultation; children; diagnostic; lung sound analysis; machine learning; mel-spectrogram; morbidity; mortality; pediatric; pneumonia; respiratory disease classification; respiratory pathology; systematic review; wheeze detection.
©Ji Soo Park, Sa-Yoon Park, Jae Won Moon, Kwangsoo Kim, Dong In Suh. Originally published in the Journal of Medical Internet Research (https://www.jmir.org), 18.04.2025.
Conflict of interest statement
Conflicts of Interest: None declared.
Figures
Similar articles
-
Automatic adventitious respiratory sound analysis: A systematic review.PLoS One. 2017 May 26;12(5):e0177926. doi: 10.1371/journal.pone.0177926. eCollection 2017. PLoS One. 2017. PMID: 28552969 Free PMC article.
-
Artificial intelligence for diagnosing exudative age-related macular degeneration.Cochrane Database Syst Rev. 2024 Oct 17;10(10):CD015522. doi: 10.1002/14651858.CD015522.pub2. Cochrane Database Syst Rev. 2024. PMID: 39417312
-
Signs and symptoms to determine if a patient presenting in primary care or hospital outpatient settings has COVID-19.Cochrane Database Syst Rev. 2022 May 20;5(5):CD013665. doi: 10.1002/14651858.CD013665.pub3. Cochrane Database Syst Rev. 2022. PMID: 35593186 Free PMC article.
-
Magnetic resonance perfusion for differentiating low-grade from high-grade gliomas at first presentation.Cochrane Database Syst Rev. 2018 Jan 22;1(1):CD011551. doi: 10.1002/14651858.CD011551.pub2. Cochrane Database Syst Rev. 2018. PMID: 29357120 Free PMC article.
-
Regional cerebral blood flow single photon emission computed tomography for detection of Frontotemporal dementia in people with suspected dementia.Cochrane Database Syst Rev. 2015 Jun 23;2015(6):CD010896. doi: 10.1002/14651858.CD010896.pub2. Cochrane Database Syst Rev. 2015. PMID: 26102272 Free PMC article.
Cited by
-
Non-invasive acoustic classification of adult asthma using an XGBoost model with vocal biomarkers.Sci Rep. 2025 Aug 6;15(1):28682. doi: 10.1038/s41598-025-14645-1. Sci Rep. 2025. PMID: 40770052 Free PMC article.
References
-
- Liu L, Oza S, Hogan D, Chu Y, Perin J, Zhu J, Lawn JE, Cousens S, Mathers C, Black RE. Global, regional, and national causes of under-5 mortality in 2000-15: an updated systematic analysis with implications for the sustainable development goals. Lancet. 2016;388(10063):3027–3035. doi: 10.1016/S0140-6736(16)31593-8. https://linkinghub.elsevier.com/retrieve/pii/S0140-6736(16)31593-8 S0140-6736(16)31593-8 - DOI - PMC - PubMed
-
- Nair H, Simões EAF, Rudan I, Gessner B, Azziz-Baumgartner E, Zhang J, Feikin DR, Mackenzie GA, Moiïsi JC, Roca A, Baggett HC, Zaman SM, Singleton RJ, Lucero MG, Chandran A, Gentile A, Cohen C, Krishnan A, Bhutta ZA, Arguedas A, Clara AW, Andrade AL, Ope M, Ruvinsky RO, Hortal M, McCracken JP, Madhi SA, Bruce N, Qazi SA, Morris SS, El Arifeen S, Weber MW, Scott JAG, Brooks WA, Breiman RF, Campbell H, Severe Acute Lower Respiratory Infections Working Group Global and regional burden of hospital admissions for severe acute lower respiratory infections in young children in 2010: a systematic analysis. Lancet. 2013;381(9875):1380–1390. doi: 10.1016/S0140-6736(12)61901-1. https://linkinghub.elsevier.com/retrieve/pii/S0140-6736(12)61901-1 S0140-6736(12)61901-1 - DOI - PMC - PubMed
-
- Aviles-Solis JC, Vanbelle S, Halvorsen PA, Francis N, Cals JWL, Andreeva EA, Marques A, Piirilä P, Pasterkamp H, Melbye H. International perception of lung sounds: a comparison of classification across some European borders. BMJ Open Respir Res. 2017;4(1):e000250. doi: 10.1136/bmjresp-2017-000250. https://bmjopenrespres.bmj.com/lookup/pmidlookup?view=long&pmid=29435344 bmjresp-2017-000250 - DOI - PMC - PubMed
-
- Ellington LE, Emmanouilidou D, Elhilali M, Gilman RH, Tielsch JM, Chavez MA, Marin-Concha J, Figueroa D, West J, Checkley W. Developing a reference of normal lung sounds in healthy Peruvian children. Lung. 2014;192(5):765–773. doi: 10.1007/s00408-014-9608-3. https://europepmc.org/abstract/MED/24943262 - DOI - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Miscellaneous
