

Comparison between norepinephrine plus epinephrine and norepinephrine plus vasopressin after return of spontaneous circulation in patients with out-of-hospital cardiac arrest
- PMID: 40251260
- PMCID: PMC12008422
- DOI: 10.1038/s41598-025-96857-z
Comparison between norepinephrine plus epinephrine and norepinephrine plus vasopressin after return of spontaneous circulation in patients with out-of-hospital cardiac arrest
Abstract
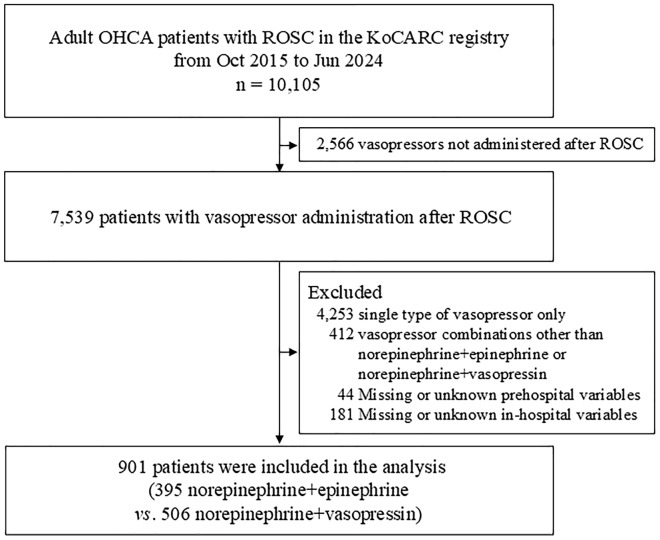
There is insufficient evidence regarding the use of second-line vasopressors following norepinephrine administration in the post-resuscitation management of patients with out-of-hospital cardiac arrest (OHCA). Therefore, this study aimed to investigate the survival outcomes between norepinephrine plus epinephrine and norepinephrine plus vasopressin as vasopressor combinations after return of spontaneous circulation (ROSC) in patients with OHCA. This retrospective observational study included data from a prospective multicenter registry. Adult patients with OHCA who achieved sustained ROSC and received vasopressor combinations of norepinephrine plus epinephrine or norepinephrine plus vasopressin were included in the study. The variable of interest was the vasopressor combination either norepinephrine plus epinephrine or norepinephrine plus vasopressin within 24 h from sustained ROSC. The primary outcome was survival to discharge. Multivariable logistic regression analysis was conducted. Between October 2015 and June 2024, 901 patients were analyzed. Survival to discharge and good neurological outcome were significantly higher in the group with norepinephrine plus epinephrine than in the group with norepinephrine plus vasopressin (17.0% vs. 9.1%, p = 0.001, and 8.1% vs. 3.2%, p = 0.002, respectively). Norepinephrine plus vasopressin was independently associated with worse survival to discharge and neurological outcome compared to norepinephrine plus epinephrine, after adjusting for potential confounders (adjusted odds ratio [aOR] 0.454, 95% confidence interval [CI] 0.277-0.746, p = 0.002 and aOR 0.346, 95% CI 0.150-0.794, p = 0.012, respectively). These findings were maintained in multiple regression models and sensitivity analyses. Norepinephrine plus epinephrine administration within 24 h from sustained ROSC showed better survival to discharge than norepinephrine plus vasopressin in patients with OHCA.
Keywords: Cardiac arrest; Epinephrine; Norepinephrine; Post-resuscitation management; Vasopressin; Vasopressor combination.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Competing interests: The authors declare no competing interests. Ethics approval and consent to participate: The Institutional Review Board of the Korea University Ansan Hospital approved this study and waived the requirement for informed consent owing to the observational nature of the study (2024AS0203). Consent for publication: The need to obtain informed consent was waived by the Institutional Review Board of the Korea University Ansan Hospital (2024AS0203).
References
-
- Odom, E. et al. Trends in EMS-attended out-of-hospital cardiac arrest survival, United States 2015–2019. Resuscitation179, 88–93. 10.1016/j.resuscitation.2022.08.003 (2022). - PubMed
-
- Atwood, C., Eisenberg, M. S., Herlitz, J. & Rea, T. D. Incidence of EMS-treated out-of-hospital cardiac arrest in Europe. Resuscitation67(1), 75–80. 10.1016/j.resuscitation.2005.03.021 (2005). - PubMed
-
- Myat, A., Song, K. J. & Rea, T. Out-of-hospital cardiac arrest: current concepts. Lancet391, 970–979. 10.1016/S0140-6736(18)30472-0 (2018). - PubMed
-
- Kiguchi, T. et al. Out-of-hospital cardiac arrest across the World: First report from the International Liaison Committee on Resuscitation (ILCOR). Resuscitation152, 39–49. 10.1016/j.resuscitation.2020.02.044 (2020). - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
