

Genotyping and refractory risk factors of mycoplasma pneumoniae pneumonia in Suzhou, China
- PMID: 40251512
- PMCID: PMC12008929
- DOI: 10.1186/s12879-025-10964-w
Genotyping and refractory risk factors of mycoplasma pneumoniae pneumonia in Suzhou, China
Abstract
Objective: To investigate the genotyping and drug resistance of Mycoplasma pneumoniae (MP) epidemic strains in children and analyze the risk factors for refractory Mycoplasma pneumoniae pneumonia (RMPP).
Method: Nasopharyngeal aspirates (NPA) were collected from hospitalized children with MP infection from September to October 2023. Tracheoscopy was performed when necessary, and Bronchoalveolar Lavage Fluid (BALF) was collected. Polymerase Chain Reaction (PCR) capillary electrophoresis were used to detect respiratory pathogens, and a nested PCR based on the MP P1 gene monitored MP subtypes. The MP-23 S rRNA V region was amplified and sequenced. Clinical data and laboratory results were analyzed for RMPP risk factors.
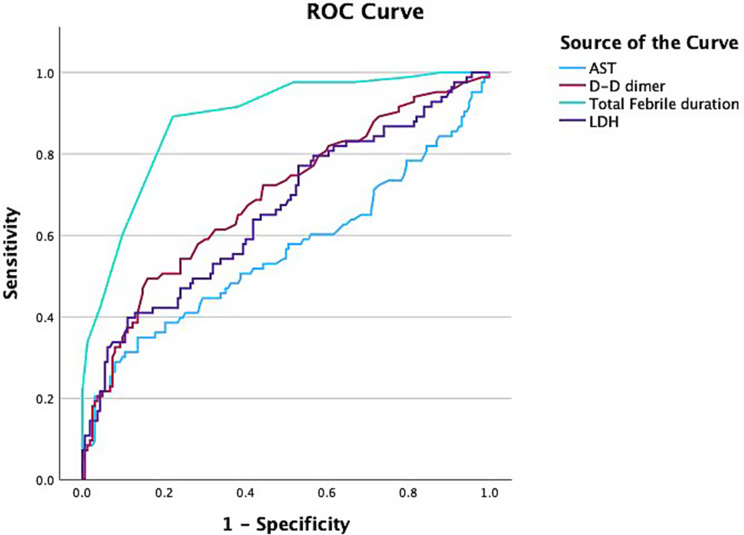
Result: From 261 children diagnosed with Mycoplasma pneumoniae pneumonia (MPP), cough (100%) and fever (93.1%) were the most common symptoms. Moist rales (65.5%) were the prevalent pulmonary signs. Bronchoscopy was required in 44.4% of cases. Drug resistance genes were detected in 258 cases (98.9%). Genotyping showed 192 cases (73.56%) as type I and 69 cases (26.4%) as type II. Type I required more bronchoscope interventions (54.2%) compared to type II (17.4%, P < 0.001). Among the children, 92 (35.2%) were classified as RMPP. The RMPP group had longer hospitalization (9.14 ± 4.38 vs. 6.7 ± 1.81 days), higher fever ratio (100% vs. 89.9%), and longer febrile duration (8.72 ± 2.52 vs. 4.56 ± 2.50 days) (all P < 0.05). Higher rates of shortness of breath (7.6% vs. 1.2%) and decreased breath sounds (30.4% vs. 16.6%) were noted in the RMPP group (P < 0.05). Additionally, higher proportions of elevated CRP, ALT, AST, LDH, and D-D dimer were found in the RMPP group, along with a greater need for bronchoscopy (70.7% vs. 43.2%). Multivariate logistic regression identified total febrile duration, mucus plug formation, elevated AST, LDH, and D-D dimer as RMPP risk factors. Receiver operator characteristic (ROC) curve indicated that total febrile duration, LDH, and D-D dimer could serve as predictive markers for RMPP.
Conclusion: Type I predominated among MP strains in Suzhou, with a high prevalence of drug resistance. Type I infections were associated with a higher likelihood of requiring bronchoscopy. Prolonged fever, mucus plug formation, elevated AST, LDH, and D-D dimer were independent risk factors for RMPP, with total febrile duration, LDH, and D-D dimer serving as predictive markers.
Clinical trial number: Not applicable.
Keywords: Drug resistance genes; Genotyping; RMPP; Risk factors.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: This study performed in accordance with the Declaration of Helsinki. All the participants’ parents or guardians gave their written informed consent for participation in the study. The study was approved by the ethics committee of Children’s hospital of Soochow University [2018CS93]. Consent for publication: Not applicable. Competing interests: The authors declare no competing interests.
Similar articles
-
Correlation between Mycoplasma pneumoniae drug resistance and clinical characteristics in bronchoalveolar lavage fluid of children with refractory Mycoplasma pneumoniae pneumonia.Ital J Pediatr. 2022 Nov 26;48(1):190. doi: 10.1186/s13052-022-01376-6. Ital J Pediatr. 2022. PMID: 36435821 Free PMC article.
-
Clinical significance of D-dimer levels in refractory Mycoplasma pneumoniae pneumonia.BMC Infect Dis. 2021 Jan 6;21(1):14. doi: 10.1186/s12879-020-05700-5. BMC Infect Dis. 2021. PMID: 33407216 Free PMC article.
-
The combination of initial markers to predict refractory Mycoplasma pneumoniae pneumonia in Chinese children: a case control study.Respir Res. 2021 Mar 22;22(1):89. doi: 10.1186/s12931-020-01577-9. Respir Res. 2021. PMID: 33752670 Free PMC article.
-
Clinical characteristics and associated factors of macrolide-resistant mycoplasma pneumoniae pneumonia in children: a systematic review and meta-analysis.Eur J Clin Microbiol Infect Dis. 2025 Jun;44(6):1505-1522. doi: 10.1007/s10096-025-05101-z. Epub 2025 Mar 19. Eur J Clin Microbiol Infect Dis. 2025. PMID: 40106136
-
Refractory Mycoplasma Pneumonia in Children: A Systematic Review and Meta-analysis of Laboratory Features and Predictors.J Immunol Res. 2022 Jun 26;2022:9227838. doi: 10.1155/2022/9227838. eCollection 2022. J Immunol Res. 2022. PMID: 35795531 Free PMC article.
References
-
- Chang CH, et al. Epidemiology and clinical manifestations of children with macrolide-resistant Mycoplasma pneumoniae pneumonia in Southern Taiwan. Pediatr Neonatol. 2021;62(5):536–42. - PubMed
-
- Xu YC, et al. Epidemiological characteristics and meteorological factors of childhood Mycoplasma pneumoniae pneumonia in Hangzhou. World J Pediatr. 2011;7(3):240–4. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
