

Median arcuate ligament syndrome in an old male: a case report with occlusion of celiac artery after stenting
- PMID: 40251574
- PMCID: PMC12007199
- DOI: 10.1186/s13019-025-03415-9
Median arcuate ligament syndrome in an old male: a case report with occlusion of celiac artery after stenting
Abstract
Background: Median arcuate ligament syndrome (MALS), also called celiac artery compression syndrome or Dunbar syndrome, is a rare disorder caused by the compression of the celiac trunk by the median arcuate ligament, which results in patients presenting with bloating, vomiting, nausea, weight loss, and postprandial abdominal pain.
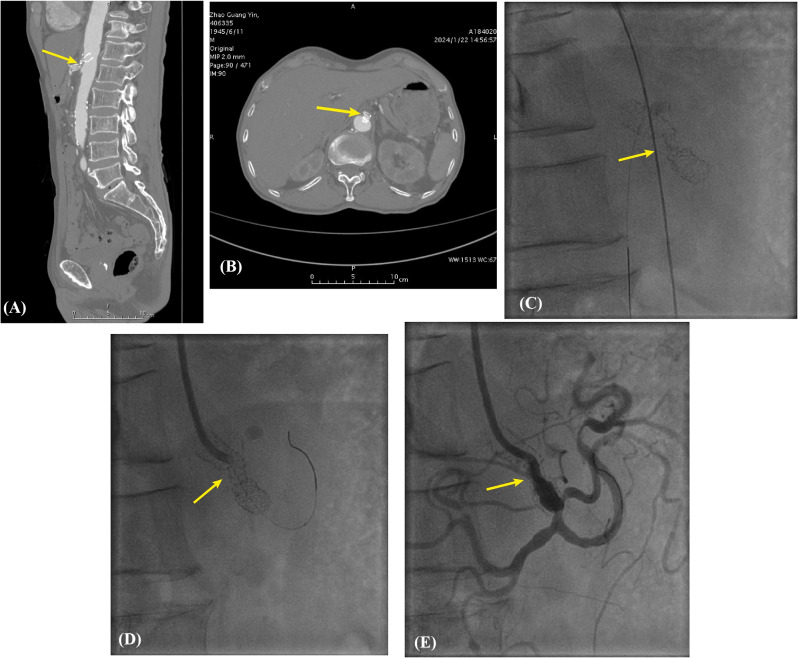
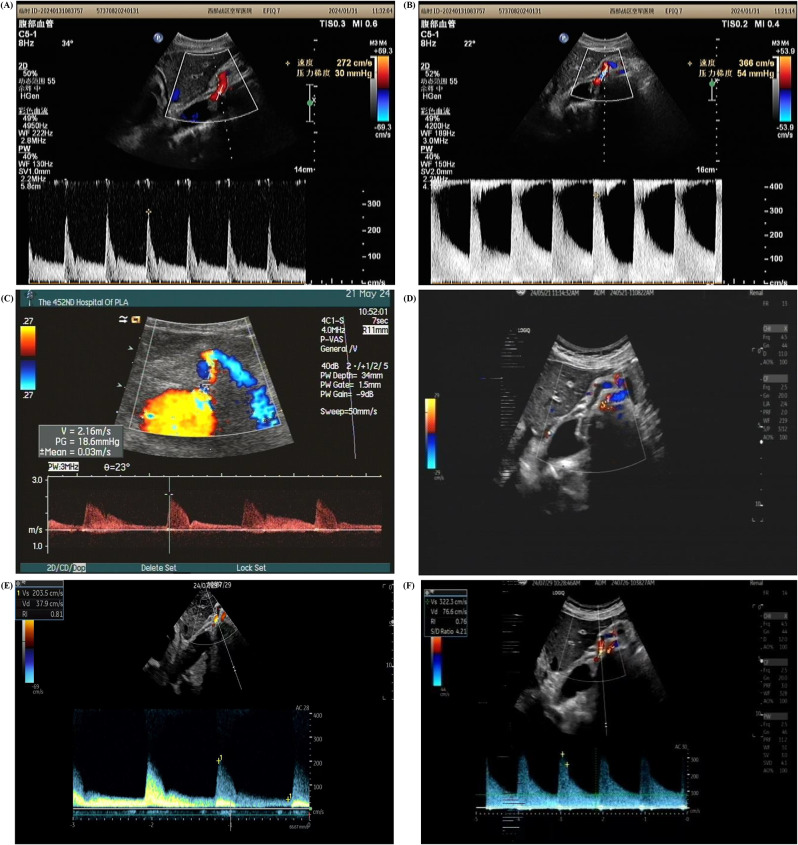
Case presentation: A 77-year-old male was admitted to our center with irregular abdominal pain over the epigastric region for the past 5 months. The pain occurred with no apparent causes, which had intensified in the last 10 days, without nausea, vomiting, and other symptoms. The physical examination, laboratory examination, abdominal ultrasound, and gastroenterological endoscope showed no obvious abnormalities. The angiography showed that the celiac artery was 90% narrowed, so revascularization was performed, leading to a resolution of the symptoms. After 6 months, the patient presented with a recurrence of abdominal pain. Computed tomography angiography showed the stent in the ostial celiac artery was compressed and deformed, which obstructed the vessel. Finally, due to the advanced age, and high surgical risk, the patient was not willing for the decompression of the celiac artery, and the post-dilation was performed, resulting in < 50% residual stenosis in the ostial celiac artery and resolution of pain.
Clinical discussion: The current diagnosis of MALS is still based on postprandial abdominal pain and imaging modalities. However, due to the atypical symptoms and imaging manifestation, MALS is diagnosed precisely only after extensive evaluation and exclusion. In our case, celiac artery stenosis was initially diagnosed based on the symptoms and the results from angiography, so the revascularization of the celiac artery was conducted, leading to the deformation of the stent and a recurrence of abdominal pain 6 months later. MALS and decompression of the celiac trunk were finally considered. Although he refused to undergo celiac artery decompression because of the high surgery risk, the abdominal pain was relieved by post-dilation during the follow-up of 8 months.
Conclusion: Due to the vague manifestation, MALS should be considered after excluding intestinal disorders using different imaging modalities. Once diagnosed, the goal of treatment was centered around the decompression of the celiac artery.
Keywords: Case report; Celiac artery compression syndrome; Dunbar syndrome; Median arcuate ligament syndrome; Vascular compression syndrome.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethical approval: Case reports are exempt from ethical approval in our institution. Informed consent: Written informed consent was obtained from the patient for publication of this case report and accompanying images. A copy of the written consent is available for review by the Editor-in-Chief of this journal on request. Competing interests: The authors declare no competing interests.
Figures
Similar articles
-
Median Arcuate Ligament Syndrome - Literature Review and Case Report.Rev Port Cir Cardiotorac Vasc. 2017 Jul-Dec;24(3-4):111. Rev Port Cir Cardiotorac Vasc. 2017. PMID: 29701344 Review.
-
Median arcuate ligament syndrome: vascular surgical therapy and follow-up of 18 patients.Langenbecks Arch Surg. 2009 Nov;394(6):1085-92. doi: 10.1007/s00423-009-0509-5. Epub 2009 Jun 9. Langenbecks Arch Surg. 2009. PMID: 19506899
-
Chronic Post-Prandial Epigastric Pain Associated with Median Arcuate Ligament Syndrome and Atherosclerosis of the Celiac Trunk in An Elderly Woman: A Case Report.Am J Case Rep. 2025 Mar 6;26:e946075. doi: 10.12659/AJCR.946075. Am J Case Rep. 2025. PMID: 40045556 Free PMC article.
-
[Diagnosis and treatment of Dunbar syndrome].Schmerz. 2024 Feb;38(1):6-11. doi: 10.1007/s00482-023-00766-x. Epub 2023 Nov 21. Schmerz. 2024. PMID: 37989790 Review. German.
-
Clinico-pathologic findings in patients with median arcuate ligament syndrome (celiac artery compression syndrome).Ann Diagn Pathol. 2021 Jun;52:151732. doi: 10.1016/j.anndiagpath.2021.151732. Epub 2021 Mar 22. Ann Diagn Pathol. 2021. PMID: 33798927 Review.
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Miscellaneous
