

Impact of pleural thickness on the sensitivity of computed tomography scan-guided cutting-needle pleural biopsy in diagnosing unexplained exudative pleural effusion
- PMID: 40251616
- PMCID: PMC12008875
- DOI: 10.1186/s12931-025-03229-2
Impact of pleural thickness on the sensitivity of computed tomography scan-guided cutting-needle pleural biopsy in diagnosing unexplained exudative pleural effusion
Abstract
Background: In most cases, patients with pleural effusion require a pleural biopsy to confirm the diagnosis, due to the low diagnostic sensitivity of thoracentesis. Among the different biopsy modalities, real time computed tomography scan-guided cutting-needle pleural biopsy (CT-CNPB) ensures high sensitivity and accessibility. However, there is no study investigating the difference in the diagnostic sensitivity of CT-CNPB for lesions with variable pleural thickness in effusions of different types.
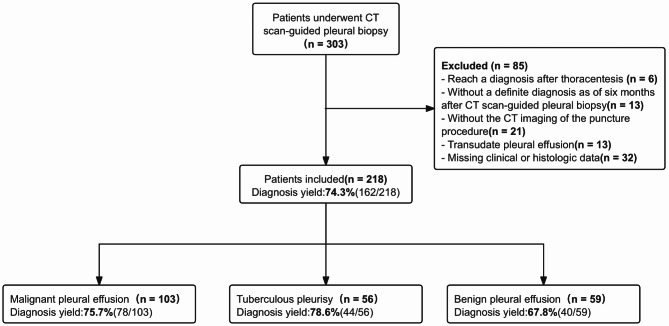
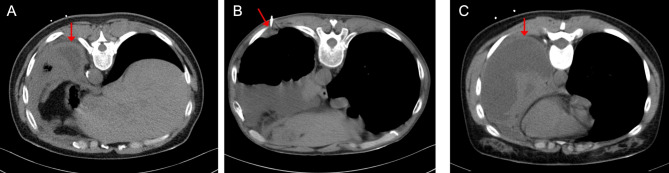
Methods: Of the 303 patients who underwent CT-CNPB, 218 met the eligibility criteria and were retrospectively analyzed from November 2021 to June 2024. Patients were divided into malignant pleural effusion (MPE), tuberculosis pleural effusion (TPE), and non-tuberculous benign pleural effusion (BPE) groups according to the diagnosis with a minimum follow-up of 6 months. Pleural thickness was defined as the length of the portion of the puncture needle that passes through the thickened parietal pleura or the pleural lesion (nodule/mass). In further analysis, we compare the differences in sensitivity between subgroups with different pleural thicknesses in each group.
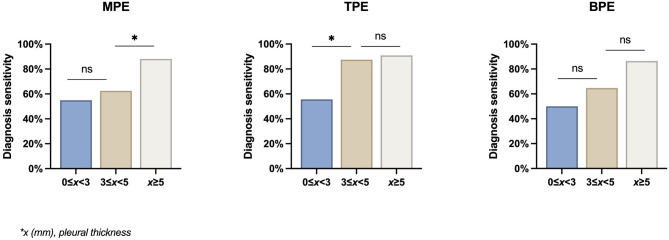
Results: The overall diagnostic sensitivity is 74.3%. The sensitivity in MPE, TPE, and BPE is 75.7%, 78.6%, and 67.8%, respectively. There was a significant difference in sensitivity between the < 5 mm and ≥ 5 mm groups in MPE and BPE groups but was not observed in the TPE group. In the further analysis, there was a significant difference in sensitivity between < 3 mm and 3-5 mm groups in TPE (p = 0.046) and a significant difference in sensitivity between 3 and 5 mm and 5-10 mm groups in MPE (p = 0.017), but a significant difference was not observed in BPE group.
Conclusion: CT-CNPB may serve as a preferred diagnostic approach in suspected TPE with pleural thickening ≥ 3 mm and suspected MPE with thickening ≥ 5 mm on chest CT. Where MT is unavailable, CT-CNPB is a viable alternative for suspected MPE or TPE patients with pleural thickening, nodularity, or mass lesions observed on CT. However, in suspected BPE, CT-CNPB alone is often insufficient; integrated clinical, laboratory, and imaging evaluation remains essential.
Keywords: Diagnosis; Exudative pleural effusion; Real time computed tomography scan-guided cutting-needle pleural biopsy.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: The study was performed in accordance with the declaration of Helsinki and was approved by the ethic committee of the West China Hospital of Sichuan University (No. 2024 − 1582). Written informed consent was waived approved by the ethic committee of the West China Hospital of Sichuan University due to the retrospective noninterventional design. Consent for publication: Not applicable. Competing interests: The authors declare no competing interests. Clinical trial number: Not applicable.
Figures
Similar articles
-
CT Scan-Guided Abrams' Needle Pleural Biopsy versus Ultrasound-Assisted Cutting Needle Pleural Biopsy for Diagnosis in Patients with Pleural Effusion: A Randomized, Controlled Trial.Respiration. 2016;91(2):156-63. doi: 10.1159/000443483. Epub 2016 Jan 19. Respiration. 2016. PMID: 26779911 Clinical Trial.
-
Ultrasound-Guided Pleural Needle Biopsy Which Needle for Which Patient: A Prospective Randomized Study.Balkan Med J. 2025 Jul 1;42(4):321-328. doi: 10.4274/balkanmedj.galenos.2025.2025-4-90. Balkan Med J. 2025. PMID: 40619802 Free PMC article. Clinical Trial.
-
Image-Assısted Pleural Needle Biopsy or Medical Thoracoscopy: Which Method for Which Patient? A Randomızed Controlled Trial.Chest. 2024 Aug;166(2):405-412. doi: 10.1016/j.chest.2024.03.038. Epub 2024 Mar 28. Chest. 2024. PMID: 38554817 Clinical Trial.
-
Evaluation of predictive value of pleural CEA in patients with pleural effusions and histological findings: A prospective study and literature review.Clin Biochem. 2016 Nov;49(16-17):1227-1231. doi: 10.1016/j.clinbiochem.2016.08.006. Epub 2016 Aug 10. Clin Biochem. 2016. PMID: 27521620 Review.
-
Image-guided pleural biopsy.Curr Opin Pulm Med. 2013 Jul;19(4):368-73. doi: 10.1097/MCP.0b013e32835f4c23. Curr Opin Pulm Med. 2013. PMID: 23719295 Review.
References
-
- Roberts ME, Rahman NM, Maskell NA, et al. British thoracic society guideline for pleural disease. Thorax. 2023;78(11):1143–56. 10.1136/thorax-2023-220304. - PubMed
-
- Rodriguez-Panadero F, Janssen JP, Astoul P. Thoracoscopy: general overview and place in the diagnosis and management of pleural effusion. Eur Respir J. 2006;28(2):409–22. 10.1183/09031936.06.00013706. - PubMed
-
- Metintas M, Ak G, Yildirim H, et al. Image-Assısted pleural needle biopsy or medical thoracoscopy: which method for which patient?? A randomızed controlled trial. Chest. 2024;166(2):405–12. 10.1016/j.chest.2024.03.038. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
