

Assessment of combined transposition of the inferior oblique muscle belly without disinsertion and contralateral inferior oblique recession for treating asymmetric inferior oblique muscle overaction (IOOA)
- PMID: 40253328
- PMCID: PMC12008889
- DOI: 10.1186/s12893-025-02882-0
Assessment of combined transposition of the inferior oblique muscle belly without disinsertion and contralateral inferior oblique recession for treating asymmetric inferior oblique muscle overaction (IOOA)
Abstract
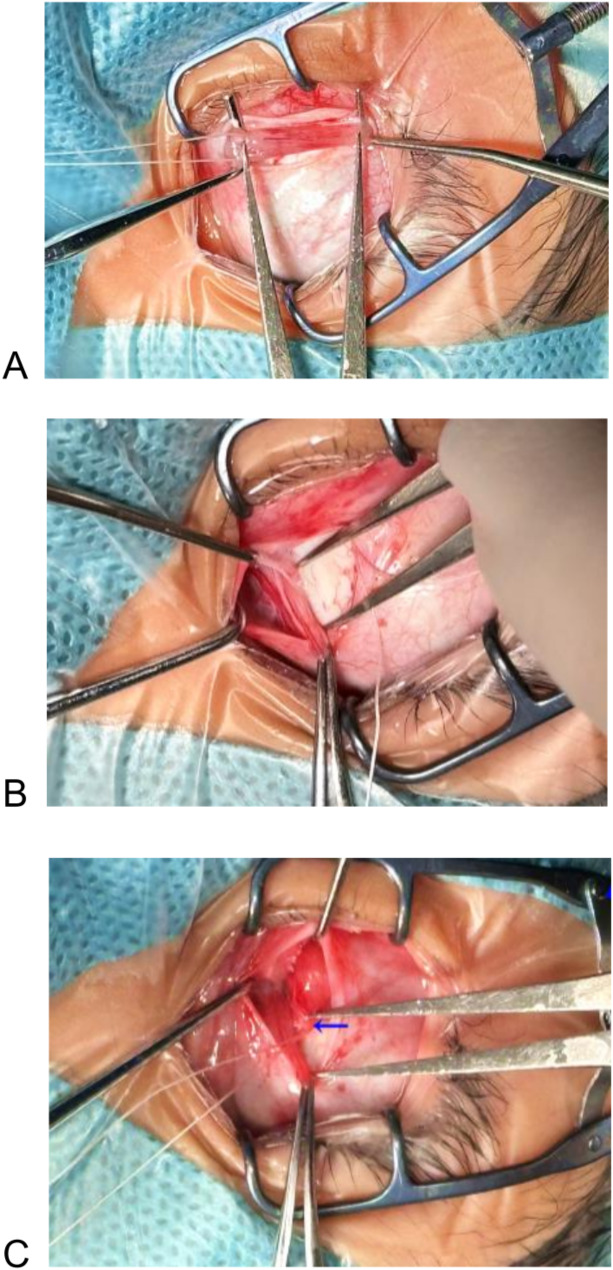
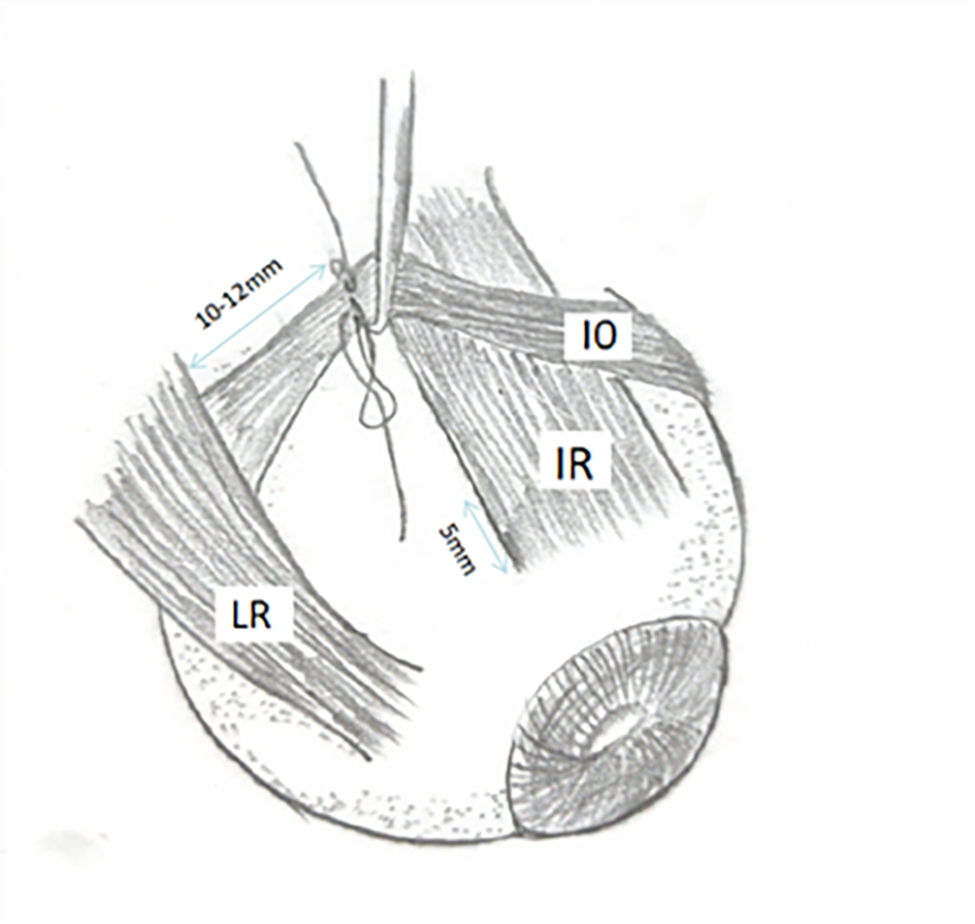
Background: This study aimed to investigate the efficacy of inferior oblique belly transposition (IOBT) combined with contralateral inferior oblique recession in treating bilateral asymmetric inferior oblique overaction (IOOA).
Methods: A retrospective study was conducted on 23 patients with asymmetric IOOA. IOBT was performed on the less affected eye of the patient, while the contralateral inferior oblique recession was conducted on the more affected eye. Pre- and post-operative changes in the vertical deviation, V-value, fovea-disc angle (FDA), and inferior oblique muscle function were compared. Follow-up duration ranged from 3 to 8 months.
Results: The V-pattern was corrected in all cases, and the V-value improved from 14.57 ± 4.50 preoperatively to 4.09 ± 2.17 postoperatively (t = 12.640, P < 0.001). The preoperative vertical deviation (5 m) significantly decreased from 8.04 ± 3.08 to 1.57 ± 1.90 postoperatively (t = 8.713, P < 0.001). Similarly, the lesser side FDA reduced from 11.39° ± 2.39° before surgery to 6.62° ± 1.11° after surgery (t = 11.132, P < 0.001). On the greater side, the FDA also showed significant improvement, reducing from 14.39° ± 2.45° preoperatively to 7.43° ± 1.23° postoperatively (t = 11.231, P < 0.001). No patients experienced anti-elevation syndrome (AES) or complications such as reverse head tilt postoperatively.
Conclusion: IOBT combined with contralateral inferior oblique recession could effectively treat asymmetric IOOA in patients with ocular asymmetry.
Keywords: Inferior oblique belly transposition; Inferior oblique muscle overaction; V-pattern exotropia.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: This study was approved by the Ethics Committee of Jinan Second People’s Hospital, and all procedures adhered to the principles outlined in the Declaration of Helsinki. Written informed consent was obtained from all participants and their parents or guardians prior to participation, confirming their understanding and agreement with the study procedures. Consent for publication: Not applicable. Competing interests: The authors declare no competing interests.
Figures
References
-
- Yang S, Guo X, Tien DR. Inferior Oblique Belly Transposition for Small Angle Hypertropia With Inferior Oblique Overaction: A Pilot Study. J Pediatr Ophthalmol Strabismus. 2018;55(1):43–46. - PubMed
-
- Awadein A, Gawdat G. Bilateral inferior oblique myectomy for asymmetric primary inferior oblique overaction. J AAPOS. 2008;12(6):560–564. - PubMed
-
- Guemes A, Wright KW. Effect of graded anterior transposition of the inferior oblique muscle on versions and vertical deviation in primary position. J AAPOS. 1998;2(4):201–206. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
