

Transcatheter arterial embolization for acute nonvariceal upper Gastrointestinal bleeding in children: a single-center retrospective study
- PMID: 40253344
- PMCID: PMC12008960
- DOI: 10.1186/s12893-025-02908-7
Transcatheter arterial embolization for acute nonvariceal upper Gastrointestinal bleeding in children: a single-center retrospective study
Abstract
Objective: This study aims to provide a preliminary report on the outcomes of transcatheter arterial embolization (TAE) in pediatric patients with acute nonvariceal upper gastrointestinal bleeding (NVUGIB) to establish optimal practices for this intervention and explore its potential value in improving the management of pediatric patients.
Methods: A retrospective analysis was conducted on children with NVUGIB who underwent TAE at a single institutional center between February 2022 and April 2024. Comprehensive data were collected, including patient demographics, clinical manifestations, diagnostic and therapeutic procedures, intraoperative findings, and follow-up outcomes.
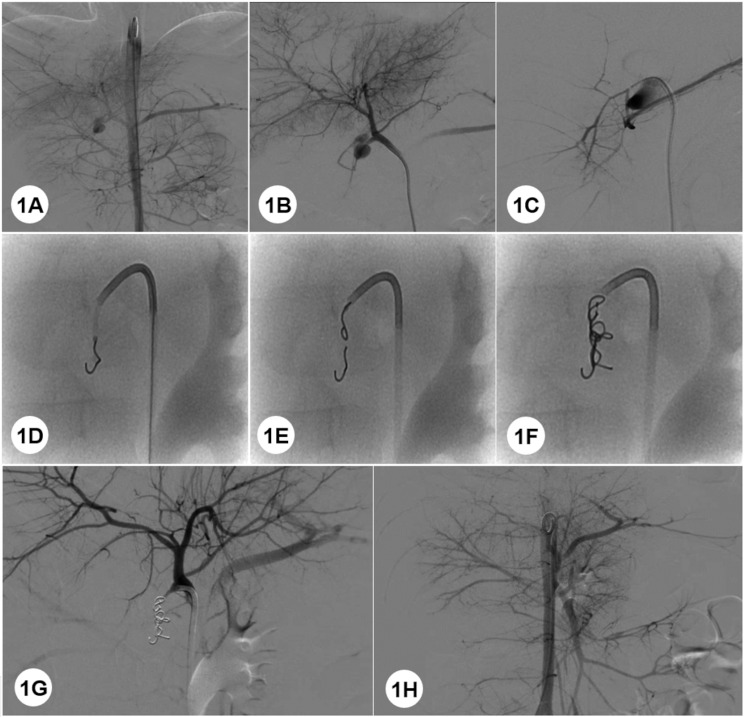
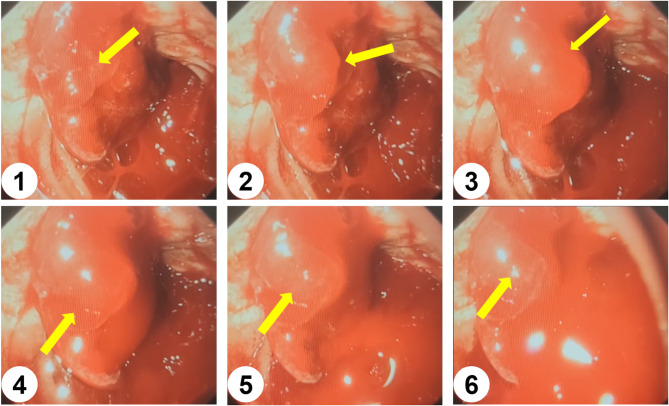
Results: A total of 266 cases with NVUGIB were admitted to the institutional center, with 14 cases (5.26%) undergoing TAE. There were 10 males and 4 females. The average age was 7.21 ± 4.77 years old, and the average hospital stay was 13.14 ± 8.69 days. Nine cases (64.29%) had hematochezia, 2 cases (14.29%) had hematemesis, 3 cases (21.42%) had both hematochezia and hematemesis. Six cases (42.86%) had no significant medical history, 3 cases (21.42%) had previous Helicobacter pylori infections, 2 cases (14.29%) had previous lymphomas, and 1 case (7.14%) each had immune disorders, gastroenteritis, and fever. The mean preoperative minimum hemoglobin level was 57.85 ± 21.25 g/L. All cases underwent gastroenteroscopy before TAE. Ten cases (71.43%) had duodenal bulb ulcers, 3 cases (21.43%) had duodenal ulcers, and 1 case (7.14%) had multiple ulcers in the gastric antrum. Bleeding was visible on endoscopy in 6 cases (Forrest Classification Ib,42.86%) (Table 2; Fig. 2), which were treated. All cases underwent TAE, and the timing of TAE averaged 4.29 ± 4.53 days. The responsible vessel was identified intraoperatively in all cases: gastroduodenal artery in 7 cases (50%) and pancreaticoduodenal artery in 7 cases (50%). A pseudoaneurysm was found in 2 cases (14.29%). Embolization of the responsible vessel was performed in all cases, using platinum coils alone in 8 cases (57.14%) and platinum coils combined with gelatin sponge in 6 cases (42.8%). All cases were followed up for an average of 13.69 ± 8.77 months, and no recurrence was detected.
Conclusion: TAE represents a promising intervention for pediatric patients with acute NVUGIB. Nevertheless, optimal timing, embolization techniques, and selection of embolizing agents necessitate further comprehensive investigation.
Keywords: Acute hemorrhage; Endoscopic; Nonvariceal upper Gastrointestinal bleeding; Pediatrics; Transcatheter arterial embolization.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethical approval: The study was ethically approved by the Fujian Provincial Maternal and Child Health Institute and approval for publication was granted. The authors have obtained all necessary patient consent forms. The patient’s guardian provided written consent for their clinical information to be reported in the journal. Conflict of interests: The authors declared no potential conflicts of interest with respect to the research, author- ship, and publication of this article.
Figures
Similar articles
-
A comparison of surgery versus transcatheter angiographic embolization in the treatment of nonvariceal upper gastrointestinal bleeding uncontrolled by endoscopy.Eur J Gastroenterol Hepatol. 2012 Aug;24(8):929-38. doi: 10.1097/MEG.0b013e32835463bc. Eur J Gastroenterol Hepatol. 2012. PMID: 22617363
-
Transcatheter arterial embolization versus surgery for refractory non-variceal upper gastrointestinal bleeding: a meta-analysis.World J Emerg Surg. 2019 Feb 1;14:3. doi: 10.1186/s13017-019-0223-8. eCollection 2019. World J Emerg Surg. 2019. PMID: 30733822 Free PMC article.
-
Diagnosis and management of nonvariceal upper gastrointestinal hemorrhage: European Society of Gastrointestinal Endoscopy (ESGE) Guideline.Endoscopy. 2015 Oct;47(10):a1-46. doi: 10.1055/s-0034-1393172. Epub 2015 Sep 29. Endoscopy. 2015. PMID: 26417980
-
Preventive transarterial embolization in upper nonvariceal gastrointestinal bleeding.World J Emerg Surg. 2017 Jan 13;12:3. doi: 10.1186/s13017-016-0114-1. eCollection 2017. World J Emerg Surg. 2017. PMID: 28101125 Free PMC article.
-
Transcatheter arterial embolization for acute nonvariceal upper gastrointestinal bleeding: Indications, techniques and outcomes.Diagn Interv Imaging. 2015 Jul-Aug;96(7-8):731-44. doi: 10.1016/j.diii.2015.05.002. Epub 2015 Jun 6. Diagn Interv Imaging. 2015. PMID: 26054245 Review.
References
-
- Rollhauser C, Fleischer D. Nonvariceal upper Gastrointestinal bleeding [J]. Endoscopy. 2001;15(1):121–33. - PubMed
-
- GRIMALDI-BENSOUDA L, ABENHAIM L. Clinical features and risk factors for upper Gastrointestinal bleeding in children: a case-crossover study [J]. Eur J Clin Pharmacol. 2010;66:831–8. - PubMed
-
- Guidelines for the diagnosis and treatment of acute non-variceal upper gastrointestinal bleeding. (2018, Hangzhou) [J]. Chinese Journal of Digestive Medicine. 2019(02):80–87. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
