

Appraising non-HDL-C, systolic pressure, and a nomogram-based diagnostic model as auxiliary biomarkers in confirming acute ischemic stroke and transient ischemic attack
- PMID: 40253553
- PMCID: PMC12009383
- DOI: 10.1038/s41598-025-97474-6
Appraising non-HDL-C, systolic pressure, and a nomogram-based diagnostic model as auxiliary biomarkers in confirming acute ischemic stroke and transient ischemic attack
Abstract
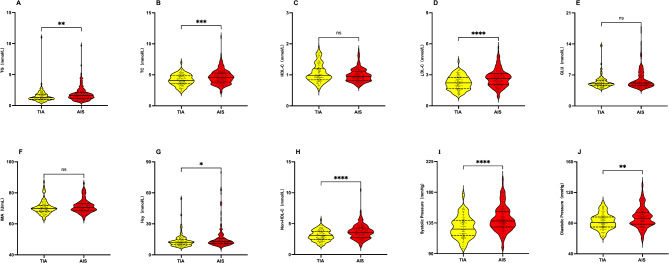
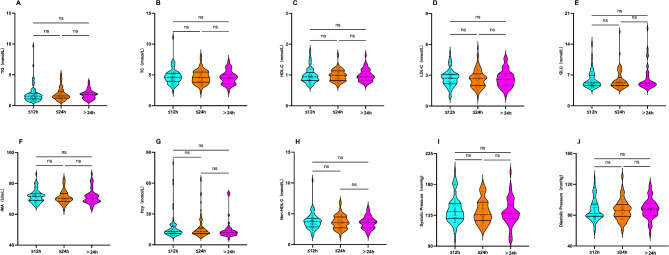
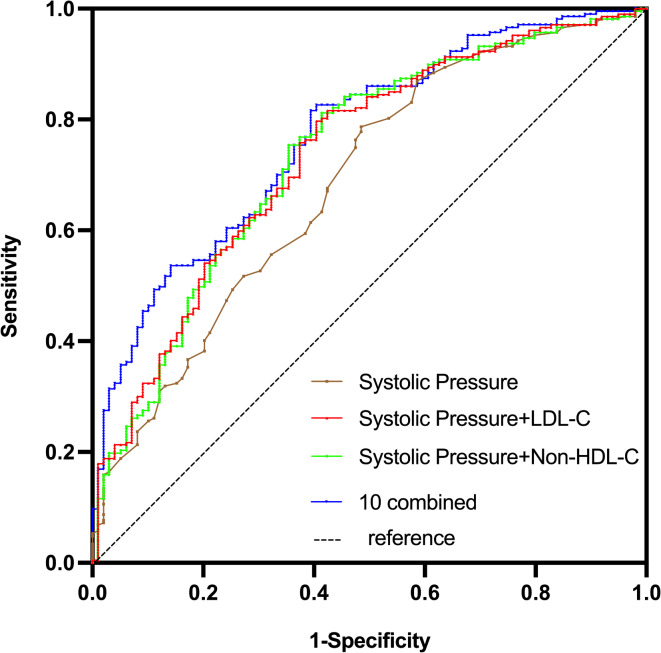
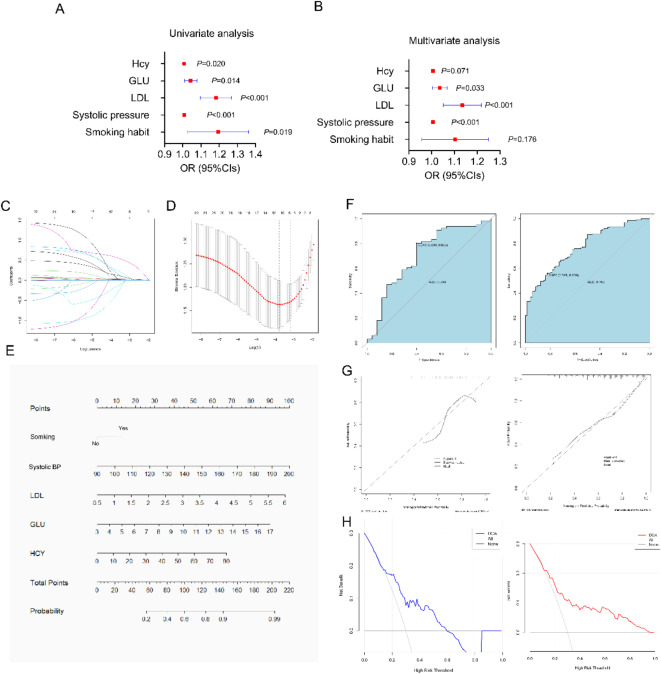
Acute ischemic stroke (AIS) is characterized by the abrupt onset of neurological dysfunction stemming from focal brain ischemia, confirmed through imaging evidence of infarction. In contrast, transient ischemic attack (TIA) manifests with neurological deficits in the absence of infarction, with imaging serving as the definitive diagnostic criterion. This study aims to assess the diagnostic value of combining non-high-density lipoprotein cholesterol (non-HDL-C) and blood pressure (BP) in differentiating AIS from TIA. We recruited 207 untreated AIS patients diagnosed within 72 h and 99 age- and gender-matched TIA patients. Upon admission, serum non-HDL-C levels, other lipid profiles, and BP measurements were obtained. Binary logistic regression was employed to identify risk factors, while receiver operator characteristic (ROC) curves were used to evaluate diagnostic performance. Furthermore, least absolute shrinkage and selection operator (LASSO) regression coupled with multivariate logistic regression was utilized to develop a nomogram model. The AIS group exhibited higher prevalence rates of hypertension, diabetes, family history of diabetes, and smoking (P < 0.05). Notably, non-HDL-C, systolic BP, diastolic BP, and other lipid markers were significantly elevated in the AIS group (P < 0.05). Multivariate analysis pinpointed non-HDL-C (OR [odds ratio] = 1.663, 95% CI [confidence interval]: 1.239-2.234, P < 0.01) and systolic BP (OR = 1.035, 95% CI: 1.012-1.057, P < 0.01) as independent risk factors. ROC analysis revealed that systolic BP alone achieved an AUC of 0.686 (sensitivity: 78.7%, specificity: 51.5%), whereas the combination of systolic BP and non-HDL-C enhanced diagnostic accuracy (AUC [area under the ROC curve] = 0.736, sensitivity: 75.4%, specificity: 64.6%). A nomogram incorporating low-density lipoprotein cholesterol (LDL-C), glucose (GLU), homocysteine, and smoking demonstrated high predictive accuracy, with training and validation AUCs of 0.769 and 0.704, respectively. Non-HDL-C and systolic BP emerge as independent risk factors for AIS, and their combined use augments diagnostic precision in differentiating AIS from TIA. A nomogram model presents a practical differentiation tool, particularly in settings with limited resources.
Keywords: Acute ischemic stroke; Non-high density lipoprotein cholesterol; Systolic pressure; Transient ischemic attack.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Competing interests: The authors declare no competing interests.
Figures
Similar articles
-
Predicting cerebral infarction and transient ischemic attack in healthy individuals and those with dysmetabolism: a machine learning approach combined with routine blood tests.Sci Rep. 2025 Apr 16;15(1):13044. doi: 10.1038/s41598-025-94682-y. Sci Rep. 2025. PMID: 40240412 Free PMC article.
-
Development and Validation of a New Nomogram Model for Predicting Acute Ischemic Stroke in Elderly Patients with Non-Valvular Atrial Fibrillation: A Single-Center Cross-Sectional Study.Clin Interv Aging. 2024 Jan 10;19:67-79. doi: 10.2147/CIA.S437065. eCollection 2024. Clin Interv Aging. 2024. PMID: 38223136 Free PMC article.
-
Correlation Analysis Between High-Density Lipoprotein Cholesterol-Carried microRNA-28-5p and Acute Ischemic Stroke.J Neurochem. 2025 Jun;169(6):e70119. doi: 10.1111/jnc.70119. J Neurochem. 2025. PMID: 40536249
-
Diagnosis and Management of Transient Ischemic Attack and Acute Ischemic Stroke: A Review.JAMA. 2021 Mar 16;325(11):1088-1098. doi: 10.1001/jama.2020.26867. JAMA. 2021. PMID: 33724327 Review.
-
Non-traditional lipid parameters as potential predictors of carotid plaque vulnerability and stenosis in patients with acute ischemic stroke.Neurol Sci. 2023 Mar;44(3):835-843. doi: 10.1007/s10072-022-06472-3. Epub 2022 Oct 27. Neurol Sci. 2023. PMID: 36301362 Review.
References
-
- Saini, V., Guada, L. & Yavagal, D. R. Global epidemiology of stroke and access to acute ischemic stroke interventions. Neurology97, S6–S16. 10.1212/wnl.0000000000012781 (2021). - PubMed
-
- Tang, X. et al. Leukoaraiosis and acute ischemic stroke. Eur. J. Neurosci.54, 6202–6213. 10.1111/ejn.15406 (2021). - PubMed
-
- Amin, H. P. et al. Diagnosis, workup, risk reduction of transient ischemic attack in the emergency department setting: A scientific statement from the American Heart Association. Stroke54, e109–e121. 10.1161/str.0000000000000418 (2023). - PubMed
-
- Patrick, L. & Halabi, C. Inpatient management of acute stroke and transient ischemic attack. Neurol. Clin.40, 33–43. 10.1016/j.ncl.2021.08.003 (2022). - PubMed
-
- Rhoney, D. H. Contemporary management of transient ischemic attack: Role of the pharmacist. Pharmacotherapy31, 193–213. 10.1592/phco.31.2.193 (2011). - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
