When Manometry and Functional Lumen Imaging Probe Disagree: The Current Limitations of the Chicago Classification Version 4.0 and Probable Extended Indications of Functional Lumen Imaging Probe
- PMID: 40254534
- PMCID: PMC12241913
- DOI: 10.5056/jnm25054
When Manometry and Functional Lumen Imaging Probe Disagree: The Current Limitations of the Chicago Classification Version 4.0 and Probable Extended Indications of Functional Lumen Imaging Probe
Abstract
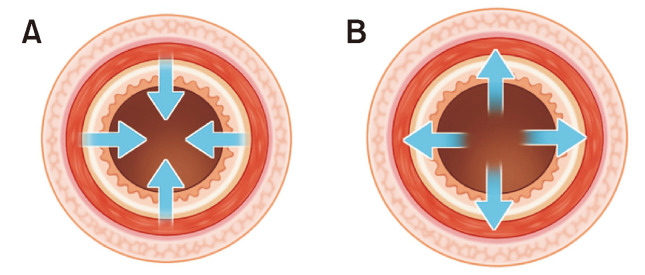
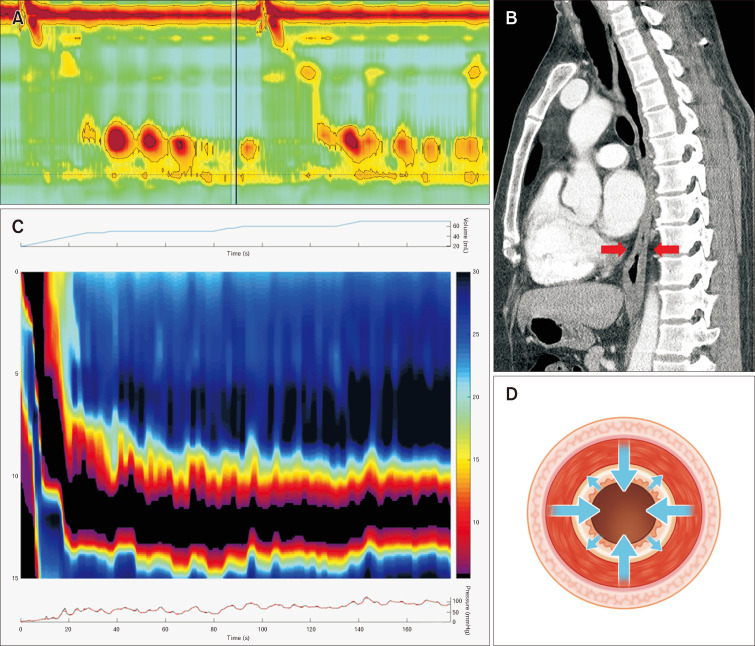
High-resolution manometry (HRM) has revolutionized evaluation of esophageal motility disorders, offering detailed pressure topography and refined diagnostic criteria codified through the Chicago classification (CC). However, patients with dysphagia may present with borderline or near-normal HRM findings, exhibiting clinically significant symptoms. CC version 4.0 (v4.0) addresses such scenarios by recommending provocative maneuvers and ancillary tests, notably functional lumen imaging probe (FLIP) and timed barium esophagography. However, growing evidence indicates that FLIP, which measures luminal distensibility under balloon distention, can detect structural or biomechanical abnormalities, such as hypertrophy or fibrosis, that remain inconspicuous on HRM. These discordant findings point to limitations in CC v4.0. FLIP complements HRM by assessing passive tissue properties and capturing balloon-induced contractility, thereby unmasking subtle esophageal wall stiffness not always reflected in integrated relaxation pressure or standard peristaltic metrics. Such discrepancies can arise in early or atypical achalasia, esophagogastric junction outflow obstruction, eosinophilic esophagitis, and even epiphrenic diverticula, where "normal" manometry may belie significant pathology. Present CC v4.0 guidelines do not specify how to incorporate FLIP-derived measures or reconcile disagreements with timed barium esophagography results, leaving certain phenotypes-including repetitive simultaneous contractions-under-recognized. These gaps underscore an overreliance on integrated relaxation pressure alone and insufficient integration of evolving FLIP technology. Thus, standardizing FLIP protocols, establishing normative distensibility data, and clarifying management pathways for manometry-FLIP discordance remain critical. Prospective, multicenter studies are needed to investigate long-term clinical outcomes and to refine how FLIP metrics can be formally integrated into future CC iterations. Ultimately, multimodal, symptom-driven approaches that leverage both HRM and FLIP are essential to fully characterize esophageal dysmotility and optimize therapy.
Keywords: Deglutition disorders; Functional lumen imaging probe; Manometry.
Conflict of interest statement
Figures
Similar articles
-
AGA Clinical Practice Update on Incorporating Functional Lumen Imaging Probe Into Esophageal Clinical Practice: Expert Review.Gastroenterology. 2025 Jul 18:S0016-5085(25)00773-5. doi: 10.1053/j.gastro.2025.05.011. Online ahead of print. Gastroenterology. 2025. PMID: 40679455
-
Interrater Reliability of Functional Lumen Imaging Probe Panometry and High-Resolution Manometry for the Assessment of Esophageal Motility Disorders.Am J Gastroenterol. 2023 Aug 1;118(8):1334-1343. doi: 10.14309/ajg.0000000000002285. Epub 2023 Apr 11. Am J Gastroenterol. 2023. PMID: 37042784 Free PMC article.
-
Enhancing Chicago Classification diagnoses with functional lumen imaging probe-mechanics (FLIP-MECH).Neurogastroenterol Motil. 2024 Aug;36(8):e14841. doi: 10.1111/nmo.14841. Epub 2024 Jun 9. Neurogastroenterol Motil. 2024. PMID: 38852150 Free PMC article.
-
The Black Book of Psychotropic Dosing and Monitoring.Psychopharmacol Bull. 2024 Jul 8;54(3):8-59. Psychopharmacol Bull. 2024. PMID: 38993656 Free PMC article. Review.
-
Esophagogastric junction distensibility assessed using the functional lumen imaging probe.World J Gastroenterol. 2017 Feb 21;23(7):1289-1297. doi: 10.3748/wjg.v23.i7.1289. World J Gastroenterol. 2017. PMID: 28275309 Free PMC article.
References
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources