

Distinct clusters of bacterial and fungal microbiota in end-stage liver cirrhosis correlate with antibiotic treatment, intestinal barrier impairment, and systemic inflammation
- PMID: 40255076
- PMCID: PMC12054929
- DOI: 10.1080/19490976.2025.2487209
Distinct clusters of bacterial and fungal microbiota in end-stage liver cirrhosis correlate with antibiotic treatment, intestinal barrier impairment, and systemic inflammation
Abstract
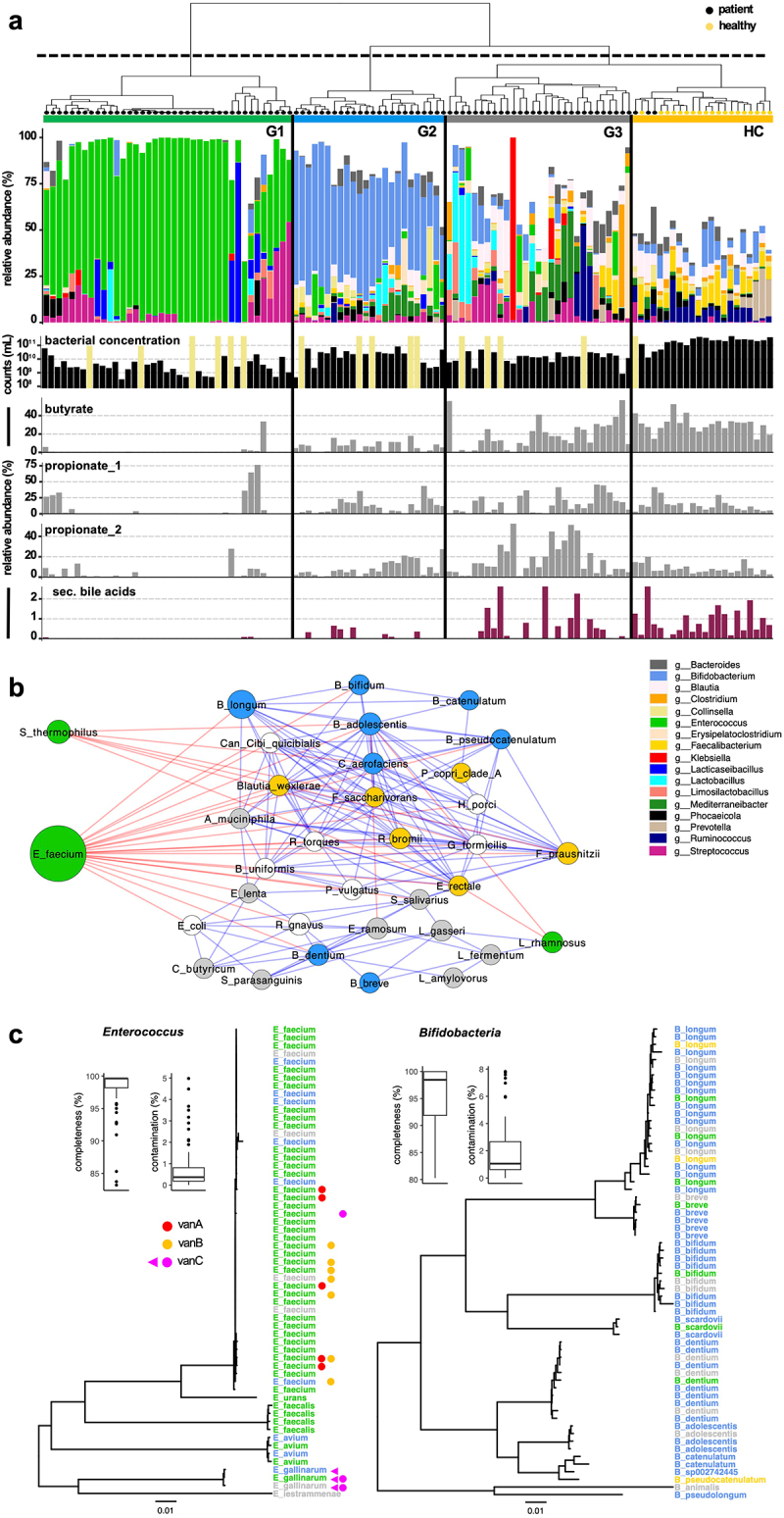
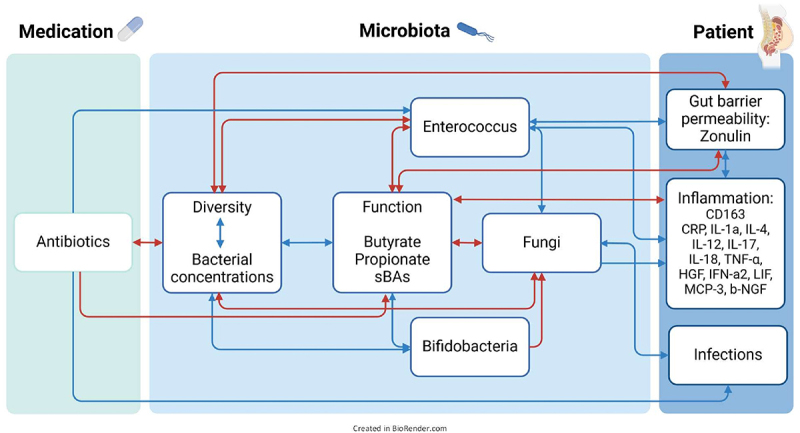
Decompensated liver cirrhosis (dLC) is associated with intestinal dysbiosis, however, underlying reasons and clinical consequences remain largely unexplored. We investigated bacterial and fungal microbiota, their relation with gut barrier integrity, inflammation, and cirrhosis-specific complications in dLC-patients. Competing-risk analyses were performed to investigate clinical outcomes within 90 days. Samples were prospectively collected from 95 dLC-patients between 2017 and 2022. Quantitative metagenomic analyses clustered patients into three groups (G1-G3) showing distinct microbial patterns. G1 (n = 39) displayed lowest diversity and highest Enterococcus abundance, G2 (n = 24) was dominated by Bifidobacteria, G3 (n = 29) was most diverse and clustered most closely with healthy controls (HC). Of note, bacterial concentrations were significantly lower in cirrhosis compared with HC, especially for G1 that also showed the lowest capacity to produce short chain fatty acids and secondary bile acids. Consequently, fungal overgrowth, dominated by Candida spp. (51.63%), was observed in G1. Moreover, G1-patients most frequently received antibiotics (n = 33; 86.8%), had highest plasma-levels of Zonulin (p = 0.044) and a proinflammatory cytokine profile along with numerically higher incidences of subsequent infections (p = 0.09). In conclusion, distinct bacterial clusters were observed at qualitative and quantitative levels and correlated with fungal abundances. Antibiotic treatment significantly contributed to dysbiosis, which translated into intestinal barrier impairment and systemic inflammation.
Keywords: Intestinal microbiome; cirrhosis-related complications; dysbiosis; fungi; gut barrier; leaky gut; liver cirrhosis; metagenomics; systemic inflammation.
Conflict of interest statement
BM served as a speaker/advisory board member for AbbVIe, Fujirebio, EWIMED, Gilead, Luvos, MSD, Norgine, Roche, W. L. Gore & Associates and received research support from Altona, EWIMED, Fujirebio, and Roche. HW served as a speaker/advisory board member for Abbott Laboratories & Abbott Molecular Inc., Bristol-Myers-Squibb, Gilead Sciences GmbH & Gilead Sciences Ltd., GlaxoSmithKline Services Unlimited, Janssen, Roche Diagnostics International Ltd., Vir Biotechnology, Inc, received research support from Abbott Laboratories & Abbott Molecular Inc., Biotest AG and received lecture fees from Biotest AG and Gilead Sciences GmbH & Gilead Sciences Ltd.
All authors declare no conflicts of interest related to this project.
Figures





References
-
- Solé C, Guilly S, Da Silva K, Llopis M, Le-Chatelier E, Huelin P, Carol M, Moreira R, Fabrellas N, De Prada G, et al. Alterations in gut microbiome in cirrhosis as assessed by quantitative metagenomics: relationship with acute-on-chronic liver failure and prognosis. Gastroenterology. 2021;160(1):206–218.e13. - PubMed
-
- Odenwald MA, Lin H, Lehmann C, Dylla NP, Cole CG, Mostad JD, Pappas TE, Ramaswamy R, Moran A, Hutchison AL, et al. Bifidobacteria metabolize lactulose to optimize gut metabolites and prevent systemic infection in patients with liver disease. Nat Microbiol. 2023;8(11):2033–2049. doi: 10.1038/s41564-023-01493-w. - DOI - PMC - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous