

BRAIN-SIM: Leveraging Simulation for Neurocritical Care Education with an Innovative Multidisciplinary Approach
- PMID: 40255088
- PMCID: PMC12177193
- DOI: 10.1177/08850666251327156
BRAIN-SIM: Leveraging Simulation for Neurocritical Care Education with an Innovative Multidisciplinary Approach
Abstract
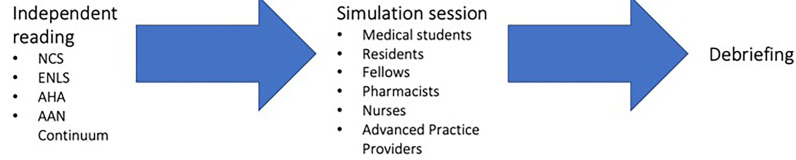
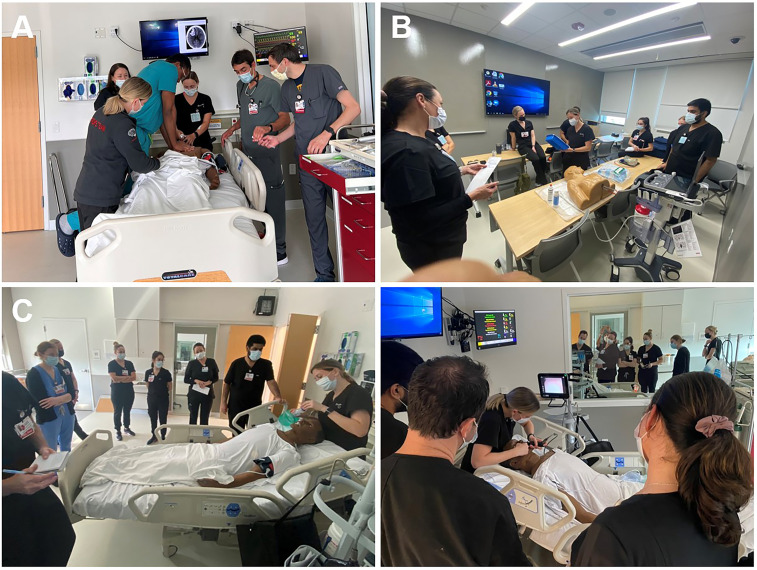
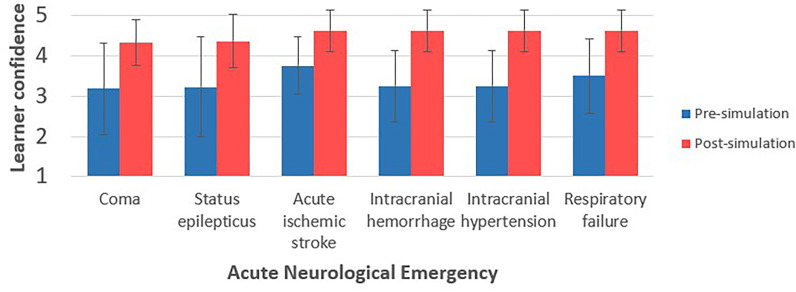
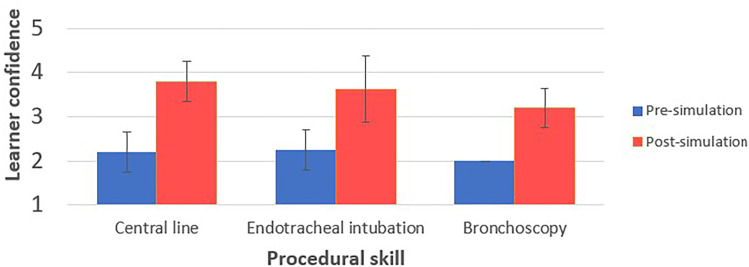
Background and ObjectivesEarly recognition and response are paramount in the treatment of neurologic emergencies. Due to its complexity, neurocritical care continues to provoke unease for practitioners and trainees. Simulation provides a realistic opportunity for learners to detect an acutely deteriorating neurologic patient and make rapid-fire treatment decisions. A multidisciplinary simulation-based learning environment may improve trainee confidence when caring for the neurocritical care patient population.MethodsNine simulation lab sessions were performed with a multidisciplinary team including medical students, residents, critical care medicine fellows, advanced practice providers (APP), critical care pharmacy residents, and neuroscience unit nurses. High fidelity manikins capable of reproducing acute neurologic and physiologic emergencies were used. After the simulation, participants completed a survey utilizing Likert scale responses regarding simulation logistics, faculty competence, and pre- and post-simulation confidence levels managing specific acute neurologic emergencies and performing neurocritical care procedural skills.ResultsNine simulation lab sessions were conducted, and thirty-eight surveys were completed. Mean learner confidence levels in managing patients improved from pre- to post-simulation in patients with coma [3.18 ± 0.51 versus 4.32 ± 0.25 (P < .001)], status epilepticus [3.23 ± 0.55 versus 4.36 ± 0.29 (P < .001)], acute ischemic stroke [3.75 ± 0.59 versus 4.63 ± 0.43 (P < .001)], intracerebral hemorrhage [3.25 ± 0.74 versus 4.63 ± 0.43 (P < .001)], intracranial hypertension [3.25 ± 0.74 versus 4.63 ± 0.43 (P < .001)], respiratory failure [3.5 ± 0.77 versus 4.63 ± 0.43 (P = .0016)], and procedures such as central lines [2.2 ± 0.56 versus 3.8 ± 0.56 (P = .003)], intubations [2.25 ± 0.39 versus 3.63 ± 0.62 (P < .001)], and bronchoscopies [2 ± 0 versus 3.2 ± 0.56 (P = .004). Consistently, learners strongly agreed that faculty were knowledgeable, well-informed, and thorough. Learners commented that the simulation experiences were realistic and allowed them to identify areas for improvement.DiscussionSimulation training can be an effective method to improve neurocritical care education by increasing clinician confidence in managing neurologic emergencies and procedures while providing opportunities for multidisciplinary collaboration. Further evaluation of the effectiveness of simulation education in this patient care setting is warranted.
Keywords: coma; confidence; critical care; education; multidisciplinary critical care; neurocritical care; simulation; status epilepticus; stroke.
Conflict of interest statement
Declaration of Conflicting InterestsThe authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Figures
Similar articles
-
Improving the Team Response to Surgical Airway Emergencies: A Simulation-based, Multidisciplinary Approach to Quality Improvement.J Surg Educ. 2025 Aug;82(8):103544. doi: 10.1016/j.jsurg.2025.103544. Epub 2025 May 15. J Surg Educ. 2025. PMID: 40378640
-
A novel simulation paradigm for medical ICU cardiopulmonary arrest training: the in situ mirror simulation.Med Educ Online. 2025 Dec;30(1):2528355. doi: 10.1080/10872981.2025.2528355. Epub 2025 Jul 3. Med Educ Online. 2025. PMID: 40607656 Free PMC article.
-
Using Real Electronic Health Records in Undergraduate Education: Roundtable Discussion.JMIR Form Res. 2025 Jun 12;9:e60789. doi: 10.2196/60789. JMIR Form Res. 2025. PMID: 40511496 Free PMC article.
-
Pharmacological and electronic cigarette interventions for smoking cessation in adults: component network meta-analyses.Cochrane Database Syst Rev. 2023 Sep 12;9(9):CD015226. doi: 10.1002/14651858.CD015226.pub2. Cochrane Database Syst Rev. 2023. PMID: 37696529 Free PMC article.
-
Assessing the comparative effects of interventions in COPD: a tutorial on network meta-analysis for clinicians.Respir Res. 2024 Dec 21;25(1):438. doi: 10.1186/s12931-024-03056-x. Respir Res. 2024. PMID: 39709425 Free PMC article. Review.
References
-
- Emergency Neurologic Life Support (ENLS) Fulfillment of ACGME Neurology Milestones [online]. https://enls.neurocriticalcare.org/enls/about/enls-residency. Accessed 10/29.
-
- Emergency Neurologic Life Support (ENLS) Fulfillment of ACGME Emergency Medicine Milestones [online]. https://enls.neurocriticalcare.org/enls/about/enls-residency. Accessed 10/29.
-
- Fanning RMM, Gaba DM. The role of debriefing in simulation-based learning. Simul Healthc: J Soc Simul Healthc. 2007;2(2):115-125. - PubMed
-
- Farias Da Guarda SN, Santos JPS, Reis MSM, et al. Realistic simulation is associated with healthcare professionals’ increased self-perception of confidence in providing acute stroke care: A before-after controlled study. Arq Neuropsiquiatr. 2021;79(1):2-7. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
