

A retrospective study on a nomogram combining clinical and ultrasound parameters for differentiating solitary parathyroid adenoma from carcinoma or atypical tumors
- PMID: 40255501
- PMCID: PMC12005988
- DOI: 10.3389/fendo.2025.1538361
A retrospective study on a nomogram combining clinical and ultrasound parameters for differentiating solitary parathyroid adenoma from carcinoma or atypical tumors
Abstract
Objective: Parathyroid carcinoma (PC) and atypical parathyroid tumor (APT) are rare malignant parathyroid disorders with varying degrees of recurrence risk. The aim of this study was to determine an effective model for discriminating PC/APT among solitary parathyroid lesions.
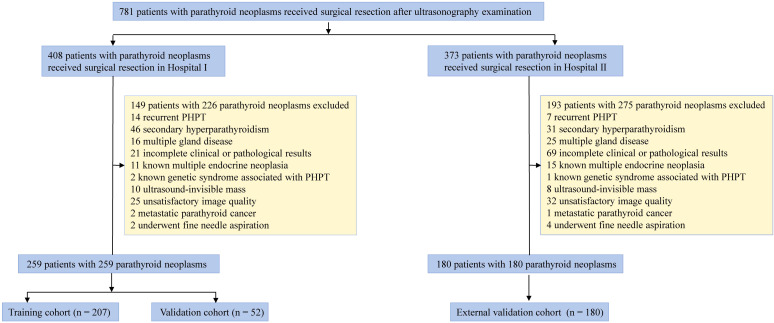
Methods: A total of 439 patients with histologically confirmed primary hyperparathyroidism were retrospectively enrolled. The training cohort comprised 207 patients, the validation cohort comprised 52 patients from Hospital I, and the external validation cohort comprised 180 patients from Hospital II. All patients were diagnosed in the parathyroid adenoma (PA) group and the APT/PC group. The clinical and ultrasonic features of the two patient groups were compared. Multivariate logistic regression analysis was conducted to identify independent risk factors for APT/PC. A nomogram was built based on multivariate logistic regression analysis. Model discrimination was assessed using receiver operating characteristic (ROC) curve analysis. The area under the curve (AUC), sensitivity, specificity, and accuracy were reported. Decision and calibration curve analyses were performed to assess the clinical value and calibration of each model, respectively.
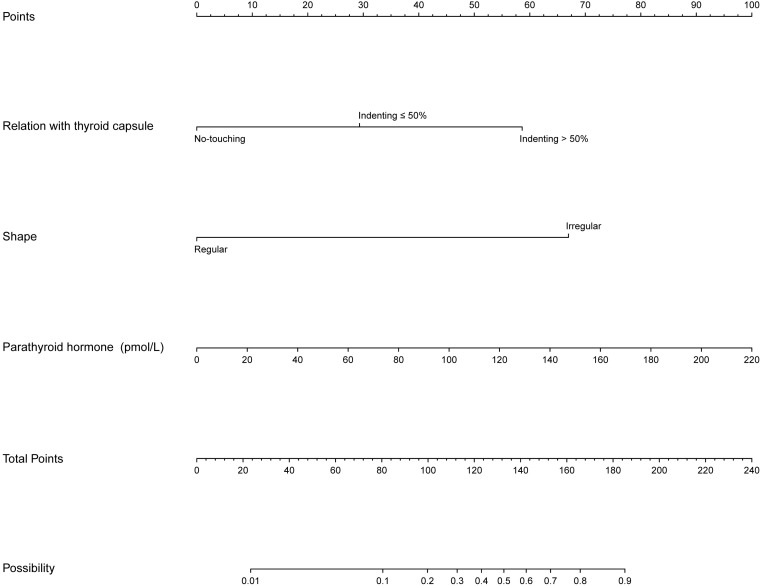
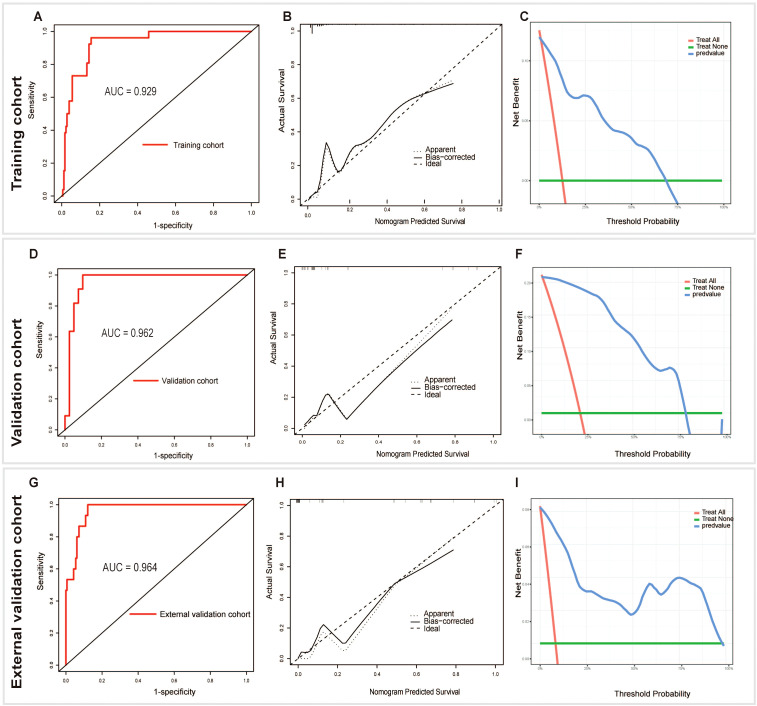
Results: In the training set, there were 181 cases of PA and 26 cases of APC/PC. Intact parathyroid hormone (iPTH) [odds ratio (OR): 1.019, 95% confidence interval (CI): 1.008-1.032], shape (OR: 16.625, 95% CI: 5.922-51.883), and relation with the thyroid capsule (OR: 3.422, 95% CI: 1.455-9.152) were independent predictive factors associated with the risk of APT/PC. The AUCs for training and internal and external validation were 0.929, 0.962, and 0.965, respectively. The accuracy, sensitivity, and specificity were 86%, 96%, and 85% in the training cohort; 92%, 100%, and 90% in the validation cohort; and 88%, 100%, and 88% in the external validation cohort, respectively. In addition, calibration plots graphically showed good agreement in the presence of the APT/PC group between risk estimation by the nomogram and histopathologic confirmation of surgical specimens. DCA in the current study showed that the nomogram was more effective than all-patient treatment or no treatment over a wide range of threshold probabilities.
Conclusions: Ultrasonic features in combination with iPTH levels may be an applicable model for predicting potentially malignant parathyroid tumors and has a better potential to facilitate preoperative decision-making.
Keywords: nomograms; parathyroid carcinoma; parathyroid neoplasms; primary hyperparathyroidism; ultrasonography.
Copyright © 2025 Liu, Li, Li, Xue, Zhang, Wei, He, Yao and Zhou.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
Ultrasound combined with biochemical parameters can predict parathyroid carcinoma in patients with primary hyperparathyroidism.Endocrine. 2019 Dec;66(3):673-681. doi: 10.1007/s12020-019-02069-7. Epub 2019 Sep 5. Endocrine. 2019. PMID: 31489590
-
Using a Novel Diagnostic Nomogram to Differentiate Malignant from Benign Parathyroid Neoplasms.Endocr Pathol. 2019 Dec;30(4):285-296. doi: 10.1007/s12022-019-09592-3. Endocr Pathol. 2019. PMID: 31734935
-
Ultrasound combined with biochemical parameters can be used to differentiate parathyroid carcinoma from benign tumors in patients with primary hyperparathyroidism.Clin Hemorheol Microcirc. 2020;76(3):351-359. doi: 10.3233/CH-200846. Clin Hemorheol Microcirc. 2020. PMID: 32675398
-
Development and validation of an ultrasound-based nomogram to improve the diagnostic accuracy for malignant thyroid nodules.Eur Radiol. 2019 Mar;29(3):1518-1526. doi: 10.1007/s00330-018-5715-5. Epub 2018 Sep 12. Eur Radiol. 2019. PMID: 30209592
-
Basic-Clinical Analysis of Parathyroid Cancer.Biomedicines. 2025 Mar 11;13(3):687. doi: 10.3390/biomedicines13030687. Biomedicines. 2025. PMID: 40149663 Free PMC article. Review.
References
MeSH terms
LinkOut - more resources
Full Text Sources