

Association between SII and postoperative pulmonary infection in elderly patients undergoing laparoscopic abdominal surgery
- PMID: 40255597
- PMCID: PMC12006073
- DOI: 10.3389/fmed.2025.1532040
Association between SII and postoperative pulmonary infection in elderly patients undergoing laparoscopic abdominal surgery
Abstract
Objectives: This study aimed to identify the contributing factors, including systemic immune-inflammation index (SII), for pulmonary infections in elderly patients undergoing laparoscopic abdominal surgery with tracheal intubation under general anesthesia.
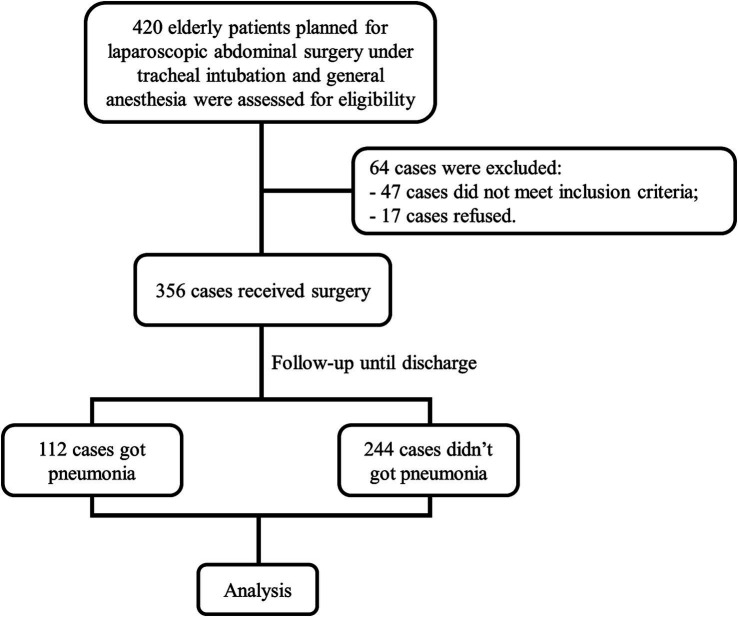
Methods: A total of 356 eligible elderly patients were monitored post-surgery for pneumonia. Pathogens were identified from sputum samples, and factors like age, smoking, chronic obstructive pulmonary disease (COPD), intubation, anesthesia duration, and SII were analyzed for their influence on infection risk.
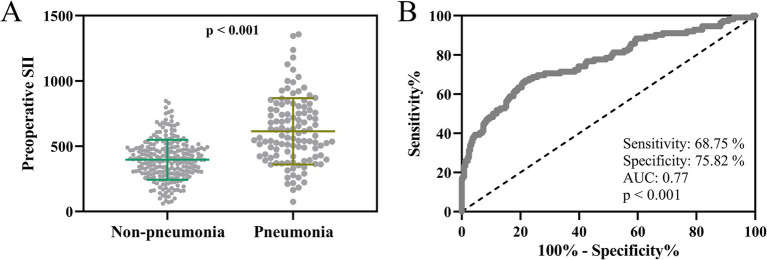
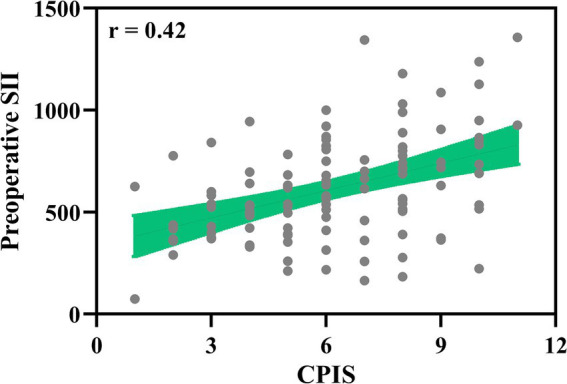
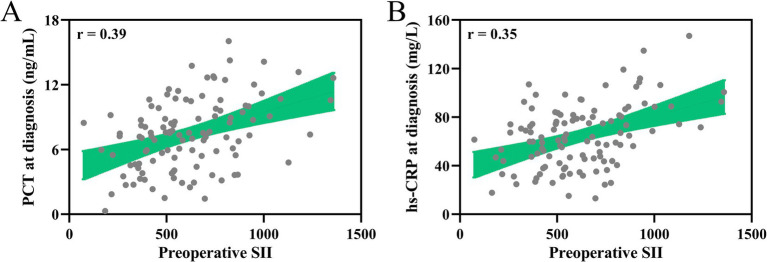
Results: The pathogens were predominantly Gram-negative bacteria, with Klebsiella pneumoniae being the most common (26%). Significant risk factors for developing pneumonia included advanced age, smoking, COPD, prolonged intubation, and extended anesthesia. A higher preoperative SII was associated with an increased risk of pneumonia and correlated with infection severity and elevated levels of inflammatory markers. Multivariate analysis identified age over 70 (OR = 1.273, p = 0.021), age over 80 (OR = 2.085, p < 0.001), COPD (OR = 1.528, p = 0.009), prolonged intubation >2 h (OR = 2.187, p < 0.001), general anesthesia >4 h (OR = 1.846, p = 0.006), operative time > 2 h (OR = 1.415, p = 0.016), and preoperative SII >489.3 (OR = 1.403, p = 0.012) as independent risk factors for postoperative pulmonary infection.
Conclusion: Our study highlighted critical risk factors for postoperative pulmonary infections in elderly patients undergoing laparoscopic abdominal surgery. Preoperative SII could be a novel predictor, offering potential for improved pre-surgical risk assessment.
Keywords: elderly patients; laparoscopic abdominal surgery; postoperative pulmonary infections; risk factors; systemic immune-inflammation index (SII).
Copyright © 2025 Wen, Kang and Shen.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
The prognostic value of red blood cell distribution width for pulmonary infection in elderly patients received abdominal surgery with tracheal intubation and general anesthesia.J Natl Med Assoc. 2023 Dec;115(6):519-527. doi: 10.1016/j.jnma.2023.09.002. Epub 2023 Oct 16. J Natl Med Assoc. 2023. PMID: 37852881
-
Predictive values of serum amyloid A, toll-like receptor 4, and sTREM-1 for ventilator-associated pneumonia in elderly patients undergoing abdominal surgery with tracheal intubation and general anesthesia.World J Surg. 2024 Oct;48(10):2383-2390. doi: 10.1002/wjs.12343. Epub 2024 Sep 19. World J Surg. 2024. PMID: 39297791
-
Systemic immune-inflammation index within the first postoperative hour as a predictor of severe postoperative complications in upper abdominal surgery: a retrospective single-center study.BMC Gastroenterol. 2022 Aug 27;22(1):403. doi: 10.1186/s12876-022-02482-9. BMC Gastroenterol. 2022. PMID: 36030214 Free PMC article.
-
Predictive significance of systemic immune-inflammation index combined with prealbumin for postoperative pneumonia following lung resection surgery.BMC Pulm Med. 2024 Jun 11;24(1):277. doi: 10.1186/s12890-024-03086-7. BMC Pulm Med. 2024. PMID: 38862955 Free PMC article.
-
Systemic immune-inflammation index for predicting postoperative atrial fibrillation following cardiac surgery: a meta-analysis.Front Cardiovasc Med. 2024 Feb 5;11:1290610. doi: 10.3389/fcvm.2024.1290610. eCollection 2024. Front Cardiovasc Med. 2024. PMID: 38374999 Free PMC article. Review.
References
-
- Perrin M, Fletcher A. Laparoscopic abdominal surgery. Continuing education in anaesthesia, critical care and pain. (2004) 4:107–10. doi: 10.1093/bjaceaccp/mkh032 - DOI
LinkOut - more resources
Full Text Sources