

Longitudinal Changes in Peripheral and Alveolar Monocyte and Inflammatory Biomarkers are Distinct in Hypercapnia Patients Following Pulmonary Sepsis-Induced ARDS
- PMID: 40255660
- PMCID: PMC12009583
- DOI: 10.2147/JIR.S508311
Longitudinal Changes in Peripheral and Alveolar Monocyte and Inflammatory Biomarkers are Distinct in Hypercapnia Patients Following Pulmonary Sepsis-Induced ARDS
Abstract
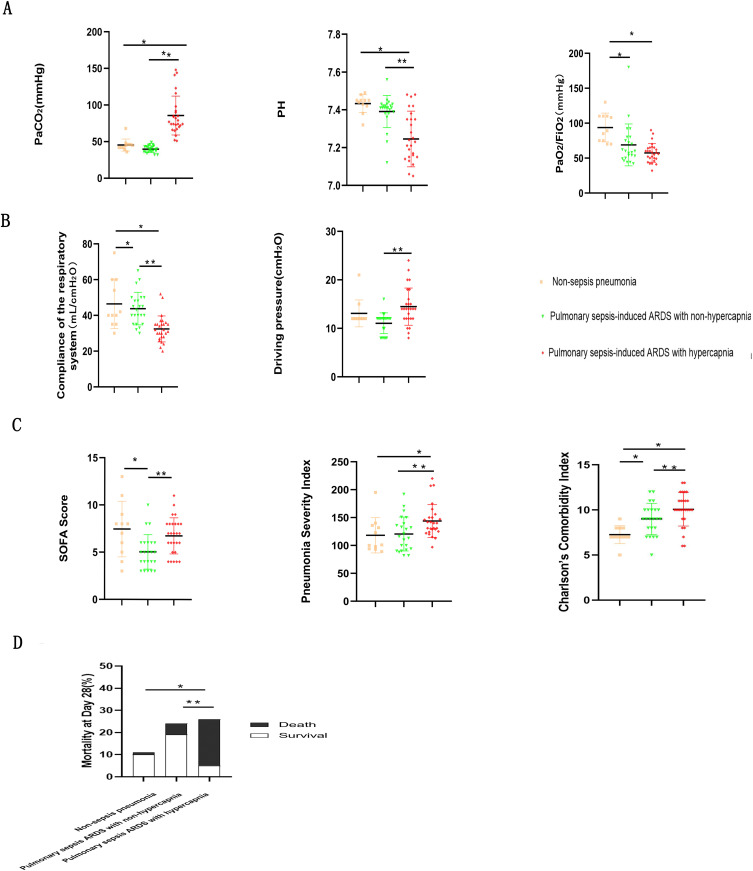
Background: Hypercapnia, an Acute Respiratory Distress Syndrome (ARDS) complication after pulmonary sepsis, remains enigmatic in terms of its immunological mechanisms. Our study was designed to compare initial values and longitudinal changes in cellular composition and inflammatory biomarkers between pneumonia sepsis-induced ARDS patients without hypercapnia and hypercapnia patients.
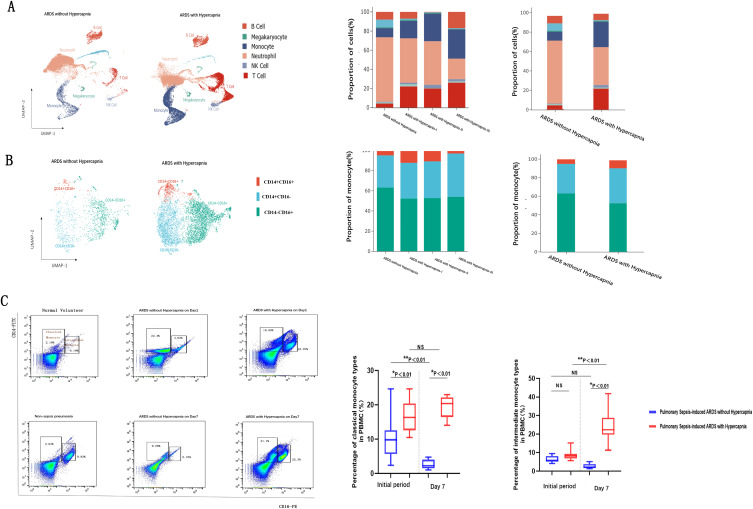
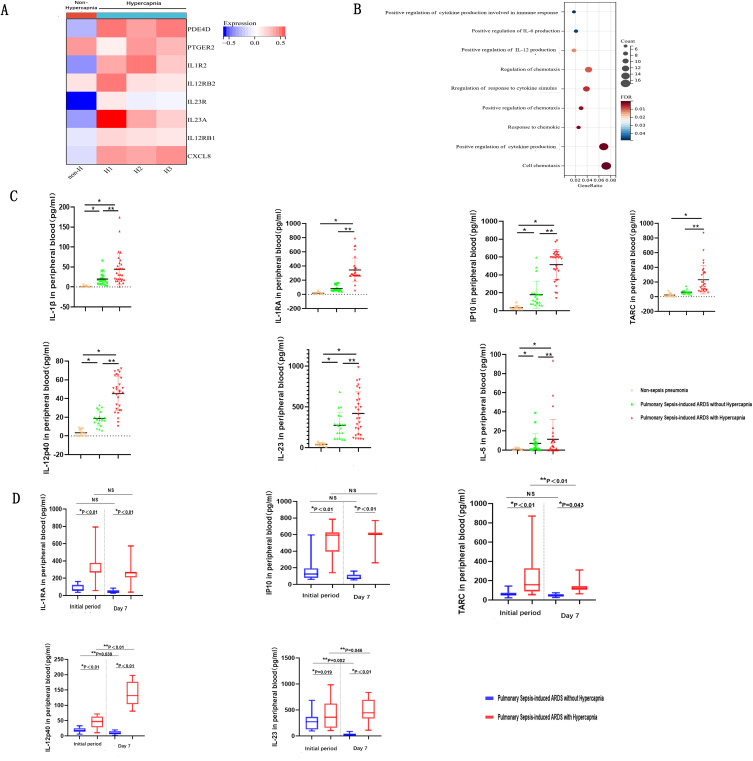
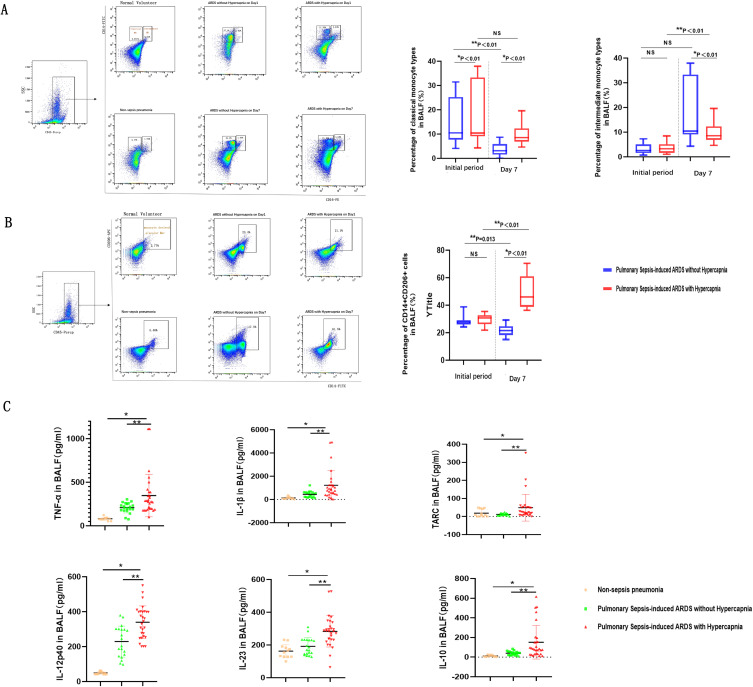
Methods: Between Dec 2022-Apr 2023, we prospectively studied 61 severe pneumonia patients. Eleven non-sepsis pneumonia patients were controls; 50 patients with pulmonary sepsis met ARDS criteria, 26 among them developed hypercapnia. We collected clinical data, respiratory parameters, peripheral blood mononuclear cells (PBMCs), and bronchoalveolar lavage fluid (BALF) at Day 1 and Day 7 post-intubation. Single-cell RNA sequencing (ScRNA-seq) was performed between selected hypercapnia and non-hypercapnia patients to characterize immune and cellular profiles. Specimens were analyzed via flow cytometry and cytokine panel.
Results: By compiling clinical data and specimens, we found that hypercapnia patients with ARDS had poorer outcomes and higher mortality. At day 1, ScRNA-seq and cytometric analysis revealed increase in monocytes and activation of cytokine storm genes with elevated interleukin (IL) -1β, IL-12p40, and IL-23 in peripheral blood. In hypercapnia patients, percentage of CD14+CD16- classical monocyte and concentrations of IL-12p40 and IL-23 increased from day 1 to day 7 in both circulation and airways. However, these alterations of cellular phenotype and cytokine decreased during seven-treatment period in non-hypercapnia patients.
Conclusion: We offer novel perspectives on monocyte-centered clusters and associated biomarkers, which play a pivotal role in driving hypercapnia after pulmonary sepsis-induced ARDS. Our study provides fresh insights into the immunological mechanisms underlying hypercapnia in ARDS, laying the foundation for useful therapeutic targets to improve patient outcomes.
Keywords: chemokine; cytokine storm; hypercapnia; monocyte; pulmonary sepsis-induced ARDS.
© 2025 Zhao et al.
Conflict of interest statement
The authors have no relevant financial or non-financial interests to disclose. This paper has been uploaded to ResearchSquare as a preprint: https://www.researchsquare.com/article/rs-4145872/v1
Figures
Similar articles
-
Alveolar compartmentalization of inflammatory and immune cell biomarkers in pneumonia-related ARDS.Crit Care. 2021 Jan 9;25(1):23. doi: 10.1186/s13054-020-03427-y. Crit Care. 2021. PMID: 33422148 Free PMC article.
-
CD14-positive extracellular vesicles in bronchoalveolar lavage fluid as a new biomarker of acute respiratory distress syndrome.Am J Physiol Lung Cell Mol Physiol. 2022 Apr 1;322(4):L617-L624. doi: 10.1152/ajplung.00052.2022. Epub 2022 Mar 2. Am J Physiol Lung Cell Mol Physiol. 2022. PMID: 35234046 Free PMC article.
-
Prediction of outcome in patients with acute respiratory distress syndrome by bronchoalveolar lavage inflammatory mediators.Exp Biol Med (Maywood). 2010 Jan;235(1):57-65. doi: 10.1258/ebm.2009.009256. Exp Biol Med (Maywood). 2010. PMID: 20404020
-
A long-lasting porcine model of ARDS caused by pneumonia and ventilator-induced lung injury.Crit Care. 2023 Jun 16;27(1):239. doi: 10.1186/s13054-023-04512-8. Crit Care. 2023. PMID: 37328874 Free PMC article. Review.
-
Acute respiratory distress syndrome heterogeneity and the septic ARDS subgroup.Front Immunol. 2023 Nov 14;14:1277161. doi: 10.3389/fimmu.2023.1277161. eCollection 2023. Front Immunol. 2023. PMID: 38035100 Free PMC article. Review.
References
-
- Katherine DW, Lorraine BW, Michael AM. Acute respiratory distress syndrome. BMJ. 2024;10(28):e076612. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
