

Fatal Acute Intestinal Obstruction with Hemophagocytic Lymphohistiocytosis and Multiple Organ Failure in Adult-Onset Still's Disease: A Rare Case Report
- PMID: 40255663
- PMCID: PMC12009564
- DOI: 10.2147/JIR.S509898
Fatal Acute Intestinal Obstruction with Hemophagocytic Lymphohistiocytosis and Multiple Organ Failure in Adult-Onset Still's Disease: A Rare Case Report
Abstract
Background: Adult-onset Still's disease (AOSD) is a systemic autoinflammatory disorder characterized by unpredictable multi-organ involvement. Although gastrointestinal complications are uncommon in AOSD, they can be life-threatening and present significant diagnostic and management challenges.
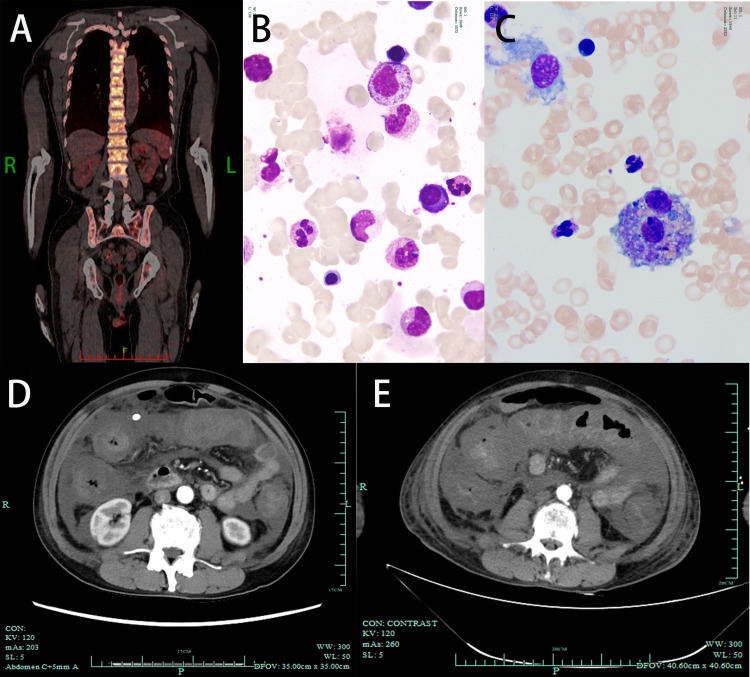
Case summary: We report the case of a 68-year-old man with AOSD who developed acute intestinal obstruction, a rare and critical complication. Imaging revealed significant colonic wall thickening, with a maximum thickness of 2.6 cm on contrast-enhanced computed tomography. The clinical status of the patient deteriorated, further complicated by the onset of hemophagocytic lymphohistiocytosis (HLH) and multi-organ failure, including acute renal dysfunction. Despite receiving intensive care and aggressive treatment, including supportive measures and immunosuppressive therapy, the patient succumbed to his illness.
Conclusion: This case underscores the importance of recognizing rare gastrointestinal and systemic complications in patients with AOSD. Early identification and prompt multidisciplinary management of conditions such as HLH and acute intestinal obstruction are essential for improving outcomes in such critical scenarios.
Keywords: acute intestinal obstruction; acute intestinal pseudo-obstruction; adult-onset Still’s disease; autoimmune disease; colonic; critical care; hemophagocytic lymphohistiocytosis; macrophage activation syndrome; multidisciplinary team (MDT); multiple organ failure.
© 2025 Li et al.
Conflict of interest statement
The authors declare that they have no competing financial interests or personal relationships that may have influenced the work reported in this study.
Figures
References
-
- Wouters JM, van de Putte LB. Adult-onset Still’s disease; clinical and laboratory features, treatment and progress of 45 cases. Q J Med. 1986;61(235):1055–1065. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
