

Acute Obstructive Hydrocephalus Due to Posterior Reversible Encephalopathy Syndrome Successfully Treated With Continuous Ventricular Drainage: A Case Report
- PMID: 40255820
- PMCID: PMC12007928
- DOI: 10.7759/cureus.80803
Acute Obstructive Hydrocephalus Due to Posterior Reversible Encephalopathy Syndrome Successfully Treated With Continuous Ventricular Drainage: A Case Report
Abstract
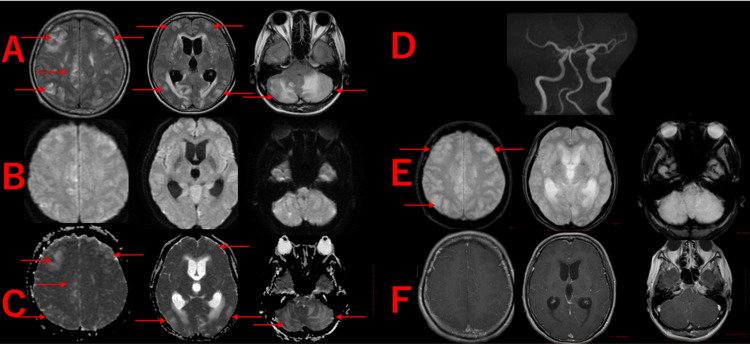
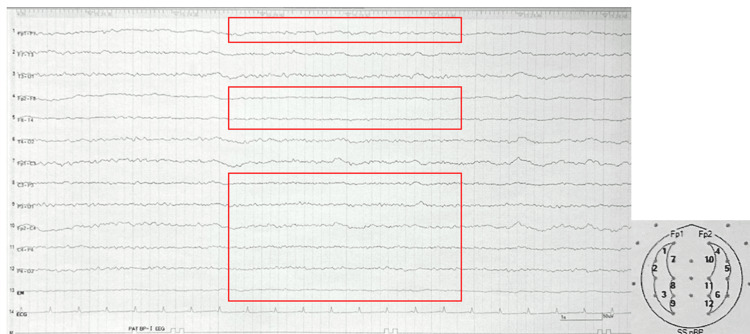
Posterior reversible encephalopathy syndrome (PRES) is an acute-onset neurological disorder characterized by various symptoms, including headache, visual disturbances, and seizures. The causes of PRES include hypertension, eclampsia, sepsis, renal failure, autoimmune diseases, and the use of chemotherapeutic agents or immunosuppressants. Although the exact pathophysiology remains unclear, it is thought to involve vasogenic edema and endothelial dysfunction. PRES generally has a favorable prognosis, and with appropriate early intervention, neurological function typically recovers without residual deficits. However, in severe cases or when diagnosis and treatment are delayed, progressive cerebral edema can lead to complications such as cerebral hemorrhage or infarction, potentially resulting in irreversible neurological deficits. In this report, we present a case of severe PRES complicated by obstructive hydrocephalus, in which early diagnosis and treatment resulted in a favorable clinical outcome without neurological deficits. A 47-year-old woman with a history of hypertension, dyslipidemia, and rheumatoid arthritis, which was in remission, had been prescribed 40 mg of nifedipine daily for hypertension. However, her medication compliance was poor, and she had discontinued antihypertensive treatment on her own approximately six months prior. Although her home-monitored systolic blood pressure (SBP) had previously averaged around 170 mmHg, it gradually increased, reaching over 200 mmHg approximately two months before admission. Two days prior to admission, she began experiencing headaches and gait disturbances, followed by seizures and impaired consciousness, prompting her emergency transport to our emergency department. Brain computed tomography (CT) and magnetic resonance imaging (MRI) revealed severe cerebral edema, most notably in the cerebellum, resulting in obstruction of the fourth ventricle and enlargement of the third and lateral ventricles, consistent with obstructive hydrocephalus. Emergency ventricular drainage was performed to prevent brain damage from elevated intracranial pressure. She was subsequently managed in the intensive care unit (ICU) with blood pressure control, sedation, and mechanical ventilation. Follow-up brain CT on day five showed improvement of cerebral edema and resolution of hydrocephalus. Her consciousness improved, and she regained the ability to walk independently, allowing discharge to her home. Although PRES generally has a good prognosis, severe cases with extensive cerebral edema may have poor outcomes. In this case, the edema was particularly prominent in the cerebellum, causing cerebrospinal fluid (CSF) outflow obstruction, which likely led to obstructive hydrocephalus. However, even in severe cases, early diagnosis and timely intervention can result in favorable clinical outcomes. In PRES, persistent severe cerebral edema may lead to obstructive hydrocephalus. In this case, early ventricular drainage and blood pressure management contributed significantly to a favorable neurological outcome. When diagnosing PRES, it is important to consider the possibility of hydrocephalus secondary to cerebral edema and to prioritize early and appropriate management of blood pressure and intracranial pressure.
Keywords: blood pressure; obstructive hydrocephalus; outcome; posterior reversible encephalopathy syndrome (pres); ventricular drainage.
Copyright © 2025, Ogino et al.
Conflict of interest statement
Human subjects: Consent for treatment and open access publication was obtained or waived by all participants in this study. Conflicts of interest: In compliance with the ICMJE uniform disclosure form, all authors declare the following: Payment/services info: All authors have declared that no financial support was received from any organization for the submitted work. Financial relationships: All authors have declared that they have no financial relationships at present or within the previous three years with any organizations that might have an interest in the submitted work. Other relationships: All authors have declared that there are no other relationships or activities that could appear to have influenced the submitted work.
Figures



References
-
- A reversible posterior leukoencephalopathy syndrome. Hinchey J, Chaves C, Appignani B, et al. N Engl J Med. 1996;334:494–500. - PubMed
-
- Posterior reversible leucoencephalopathy syndrome: Case series, comments, and diagnostic dilemma. Chaudhuri J, Basu S, Roy MK, Chakravarty A. Curr Neurol Neurosci Rep. 2023;23:433–449. - PubMed
-
- 2014 evidence-based guideline for the management of high blood pressure in adults: Report from the panel members appointed to the Eighth Joint National Committee (JNC 8) James PA, Oparil S, Carter BL, et al. JAMA. 2014;311:507–520. - PubMed
Publication types
LinkOut - more resources
Full Text Sources