

Real-World Study of Systemic Treatment after First-Line Atezolizumab plus Bevacizumab for Hepatocellular Carcinoma in Asia-Pacific Countries
- PMID: 40255875
- PMCID: PMC12005689
- DOI: 10.1159/000540969
Real-World Study of Systemic Treatment after First-Line Atezolizumab plus Bevacizumab for Hepatocellular Carcinoma in Asia-Pacific Countries
Abstract
Introduction: Atezolizumab plus bevacizumab is a commonly used first-line regimen for advanced hepatocellular carcinoma (HCC) treatment owing to its superior outcomes compared to sorafenib. However, optimal subsequent treatment options for patients with HCC who progressed on first-line atezolizumab plus bevacizumab remain unclear.
Methods: This multinational, multi-institutional, retrospective study included patients with HCC from 22 centers in five Asia-Pacific countries who were treated with first-line atezolizumab plus bevacizumab, which was discontinued for any reason. The endpoints included progression-free survival (PFS) and overall survival (OS) according to patient characteristics and second-line regimens.
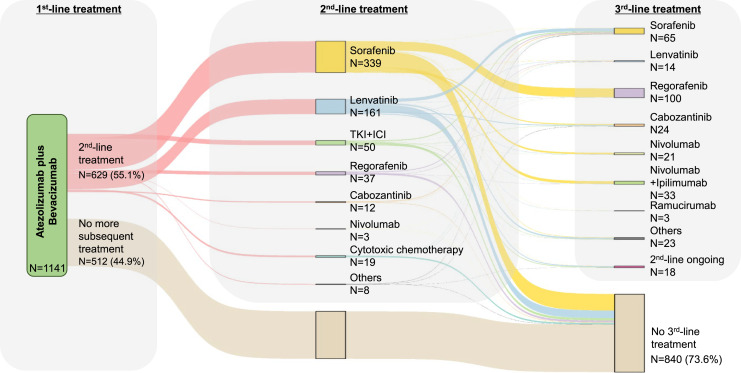
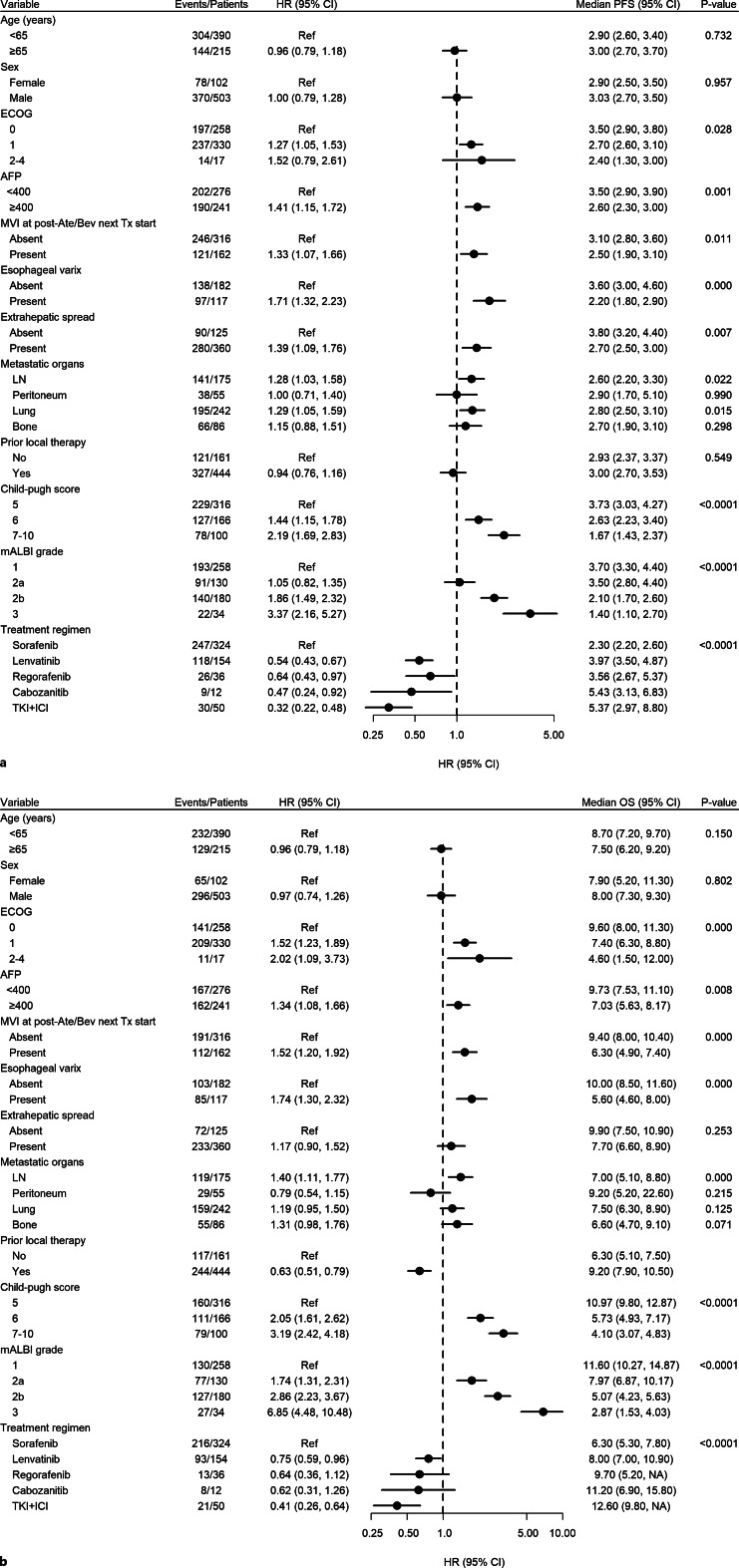
Results: Between June 2016 and May 2023, 1,141 patients were treated with first-line atezolizumab plus bevacizumab, of whom 629 (55.1%) received subsequent treatment. Sorafenib and lenvatinib were the most commonly administered second-line regimens (53.9% and 25.6%, respectively). Overall, the median PFS and OS were 2.9 and 8.0 months, respectively. Lenvatinib had longer PFS (4.0 vs. 2.3 months) and OS (8.0 vs. 6.3 months) than sorafenib. Patients treated with tyrosine kinase inhibitor (TKI) plus immune checkpoint inhibitor (ICI) (n = 50, 8.3%) showed PFS and OS of 5.4 and 12.6 months, respectively. Lower tumor burden and lenvatinib or TKI plus ICI use were associated with longer second-line PFS. Preserved liver function was associated with improved OS.
Conclusions: In patients with HCC who progressed on first-line atezolizumab plus bevacizumab, sorafenib and lenvatinib were the most commonly used second-line regimens in Asia-Pacific countries, with lenvatinib resulting in longer OS than sorafenib. The second-line TKI plus ICI combination exhibited promising efficacy, suggesting the potential role of continuing ICIs beyond disease progression.
Keywords: Asia-Pacific; Atezolizumab plus bevacizumab; Hepatocellular carcinoma; Real-world data; Second-line treatment.
© 2024 The Author(s). Published by S. Karger AG, Basel.
Conflict of interest statement
C.-k.L. received honoraria from AstraZeneca, Servier, Dong-A ST, Boryung Pharmaceuticals, and Roche; consulting fees from Roche and Daiichi Sankyo; and research grants or supports from Ono Pharmaceuticals, Celltrion, Boryung Pharmaceuticals, GC Biopharma, and Lunit Inc. C.Y. received honoraria from Servier, Bayer, AstraZeneca, Merck Sharp & Dohme, Eisai, Celgene, Bristol Myers Squibb, Ipsen, Novartis, Boryung Pharmaceuticals, Mundipharma, and Roche and research grants from Servier, Bayer, AstraZeneca, Ono Pharmaceuticals, Ipsen, Boryung Pharmaceuticals, and Lunit Inc. R.S. is on an advisory board for and receives honoraria for talks from Bristol Myers Squibb; is on an advisory board for and receives fees for travel from Eisai; is on an advisory board for and receives fees for talks and travel from Taiho and DiethelmKellerSiberHegner; is on an advisory board for and receives fees for talks and research funding from Merck Sharp & Dohme; is on an advisory board for Merck, Bayer, Novartis, GlaxoSmithKline, Astellas, Pierre-Fabre, and Tavotek; receives honoraria for talks from Eli Lilly; receives honoraria for talks and travel from Roche, AstraZeneca, and Ipsen; receives research funding and patents from Paxman Coolers; receives research funding from Natera; receives patents from Auristone, outside the submitted work; and has pending patents with Auristone and Paxman. S.L.C. serves as an advisory member for AstraZeneca, MSD, Eisai, BMS, Ipsen, and Hengrui and received research funds from MSD, Eisai, Ipsen, SIRTEX, and Zailab and honoraria from AstraZeneca, Eisai, Roche, Ipsen, and MSD. Hong Jae Chon has a consulting or advisory role at Eisai, Roche, Bayer, ONO, MSD, BMS, Celgene, Sanofi, Servier, AstraZeneca, and GreenCross Cell and has received research grants from Roche, Dong-A ST, and Boryung Pharmaceuticals. The other authors have no conflicts of interest to declare.
Figures


References
-
- Llovet JM, Kelley RK, Villanueva A, Singal AG, Pikarsky E, Roayaie S, et al. . Hepatocellular carcinoma. Nat Rev Dis Primers. 2021;7(1):6. - PubMed
-
- Chan SL, Wong VW, Qin S, Chan HL. Infection and cancer: the case of hepatitis B. J Clin Oncol. 2016;34(1):83–90. - PubMed
-
- Bertuccio P, Turati F, Carioli G, Rodriguez T, La Vecchia C, Malvezzi M, et al. . Global trends and predictions in hepatocellular carcinoma mortality. J Hepatol. 2017;67(2):302–9. - PubMed
-
- Llovet JM, Ricci S, Mazzaferro V, Hilgard P, Gane E, Blanc JF, et al. . Sorafenib in advanced hepatocellular carcinoma. N Engl J Med. 2008;359(4):378–90. - PubMed
LinkOut - more resources
Full Text Sources
