

Social determinants of recovery from ongoing symptoms following COVID-19 in two UK longitudinal studies: a prospective cohort study
- PMID: 40256447
- PMCID: PMC12007038
- DOI: 10.1136/bmjph-2024-001166
Social determinants of recovery from ongoing symptoms following COVID-19 in two UK longitudinal studies: a prospective cohort study
Abstract
Introduction: Social gradients in COVID-19 exposure and severity have been observed internationally. Whether combinations of pre-existing social factors, particularly those that confer cumulative advantage and disadvantage, affect recovery from ongoing symptoms following COVID-19 and long COVID is less well understood.
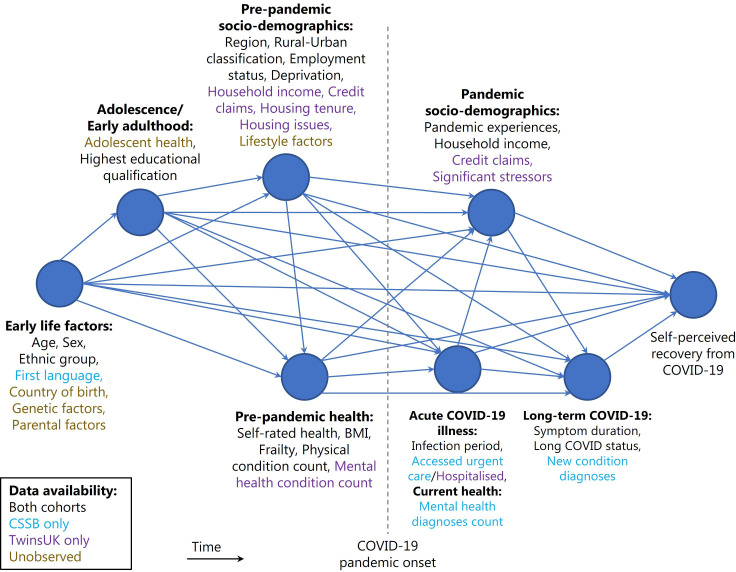
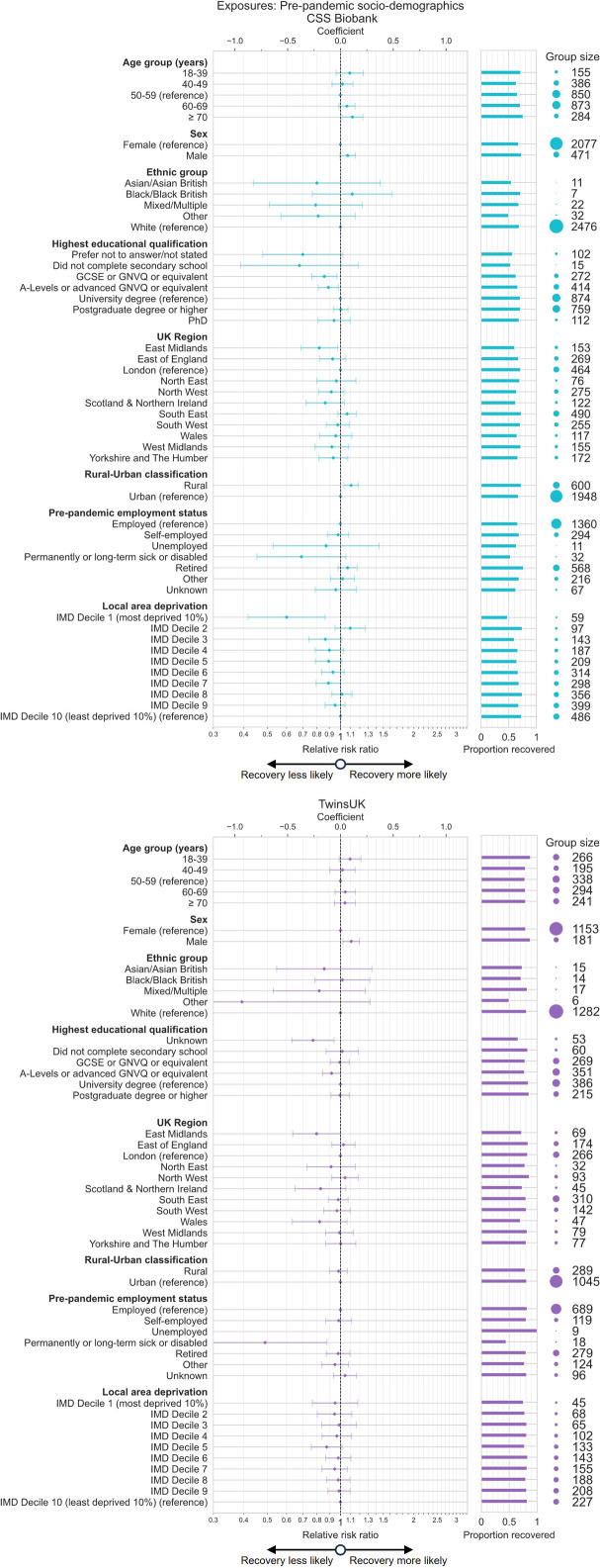
Methods: We analysed data on self-perceived recovery following self-reported COVID-19 illness in two UK community-based cohorts, COVID Symptom Study Biobank (CSSB) (N=2548) and TwinsUK (N=1334). Causal effects of sociodemographic variables reflecting status prior to the COVID-19 pandemic on recovery were estimated with multivariable Poisson regression models, weighted for inverse probability of questionnaire participation and COVID-19 infection and adjusted for potential confounders. Associations between recovery and social strata comprising combinations of sex, education level and local area deprivation were estimated using the intersectional multilevel analysis of individual heterogeneity and discriminatory accuracy (MAIHDA) approach. Further analyses estimated associations with variables reflecting experiences during the pandemic.
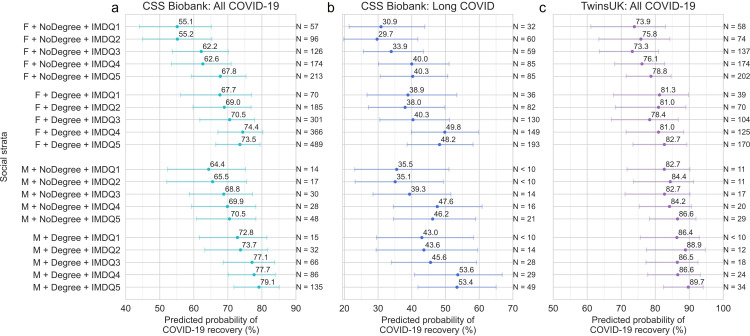
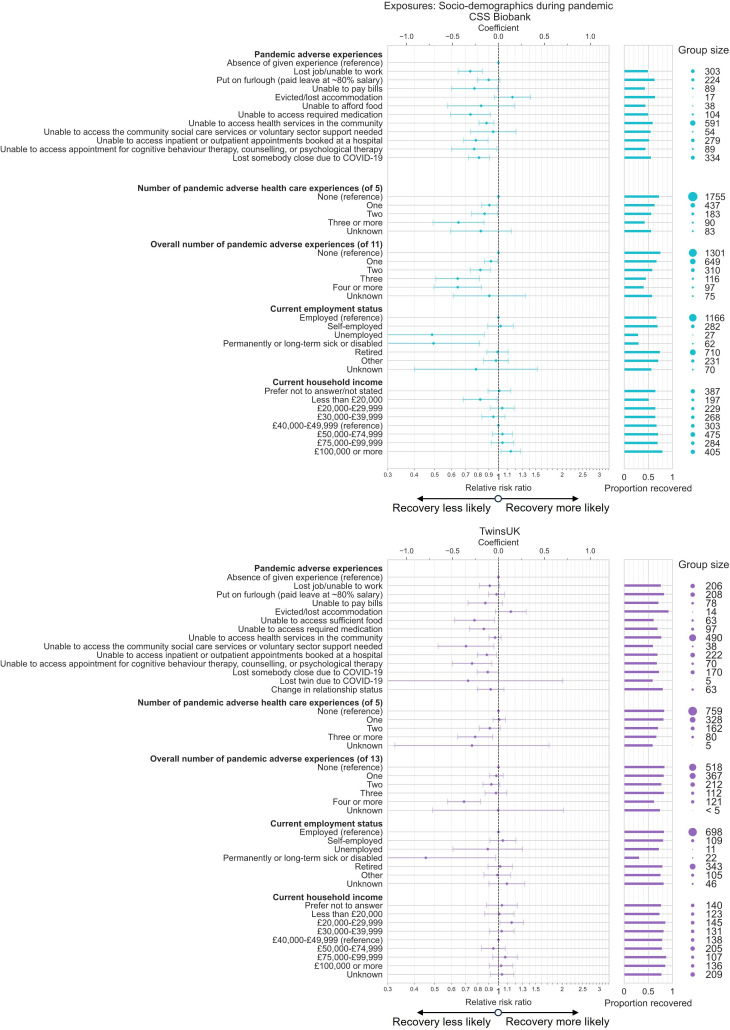
Results: Gradients in recovery from COVID-19 along the lines of social advantage were observed in intersectional MAIHDA models, with predicted probability of recovery lowest in female strata with lowest education and highest deprivation levels (CSSB: 55.1% (95% CI 44.0% to 65.1%); TwinsUK: 73.9% (95% CI 61.1% to 83.0%)) and highest in male strata with highest education and lowest deprivation levels (CSSB: 79.1% (95% CI 71.8% to 85.1%); TwinsUK: 89.7% (95% CI 82.5% to 94.1%)). Associations were not explained by differences in prepandemic health. Adverse employment, financial, healthcare access and personal experiences during the pandemic were also negatively associated with recovery.
Conclusions: Inequalities in likelihood of recovery from COVID-19 were observed, with ongoing symptoms several months after coronavirus infection more likely for individuals with greater social disadvantage prior to the pandemic.
Keywords: COVID-19; SARS-CoV-2; Social Medicine; Sociodemographic Factors.
Copyright © Author(s) (or their employer(s)) 2025. Re-use permitted under CC BY. Published by BMJ Group.
Conflict of interest statement
NJC is supported by NIHR via their institution. MPG is supported by UKRI and NIHR via their institution, is chair of the TwinsUK Volunteer Advisory Board, and declares accommodation and registration fees paid for by conference organisers for International Society for Twin Studies (ISTS); Twins Congress 2023. JDC is supported by NIHR via their institution. AG is supported by a UKRI Future Leaders Fellowship. EJT is supported by NIHR via their institution, and project grants from NIHR and EU Hospital Association. CHS is supported by Alzheimer’s Society via their institution, is Scientific Advisor to and stock holder in BrainKey. EM is supported by NIHR and MRC via their institution. MA is supported by NIHR via their institution. RSP was supported by an NIHR Academic Clinical Fellowship and is currently supported by a Wellcome Trust Personal PhD fellowship grant. NRH is supported by NIHR via their institution. LSC is supported by Wellcome Trust. BM is supported by NIHR via their institution. EK is supported by Wellcome EPSRC Centre for Medical Engineering via their institution. SO is supported by NIHR via their institution. ELD was supported by Chronic Disease Research Foundation via their institution. CJS is supported by UKRI and NIHR via their institution, and previously consulted for ZOE Ltd. All other authors have nothing to declare.
Figures
Similar articles
-
Antibody tests for identification of current and past infection with SARS-CoV-2.Cochrane Database Syst Rev. 2022 Nov 17;11(11):CD013652. doi: 10.1002/14651858.CD013652.pub2. Cochrane Database Syst Rev. 2022. PMID: 36394900 Free PMC article.
-
Rapid, point-of-care antigen tests for diagnosis of SARS-CoV-2 infection.Cochrane Database Syst Rev. 2022 Jul 22;7(7):CD013705. doi: 10.1002/14651858.CD013705.pub3. Cochrane Database Syst Rev. 2022. PMID: 35866452 Free PMC article.
-
Signs and symptoms to determine if a patient presenting in primary care or hospital outpatient settings has COVID-19.Cochrane Database Syst Rev. 2022 May 20;5(5):CD013665. doi: 10.1002/14651858.CD013665.pub3. Cochrane Database Syst Rev. 2022. PMID: 35593186 Free PMC article.
-
How lived experiences of illness trajectories, burdens of treatment, and social inequalities shape service user and caregiver participation in health and social care: a theory-informed qualitative evidence synthesis.Health Soc Care Deliv Res. 2025 Jun;13(24):1-120. doi: 10.3310/HGTQ8159. Health Soc Care Deliv Res. 2025. PMID: 40548558
-
SARS-CoV-2-neutralising monoclonal antibodies for treatment of COVID-19.Cochrane Database Syst Rev. 2021 Sep 2;9(9):CD013825. doi: 10.1002/14651858.CD013825.pub2. Cochrane Database Syst Rev. 2021. PMID: 34473343 Free PMC article.
References
-
- WHO Post COVID-19 condition (Long COVID) [5-Jan-2023]. https://www.who.int/europe/news-room/fact-sheets/item/post-covid-19-cond... Available. Accessed.
-
- NICE Overview | COVID-19 rapid guideline: managing the long-term effects of COVID-19 | Guidance | NICE. [10-Oct-2022]. https://www.nice.org.uk/guidance/ng188 Available. Accessed.
-
- CDC Post-COVID Conditions: Information for Healthcare Providers. [1-Mar-2023]. https://www.cdc.gov/coronavirus/2019-ncov/hcp/clinical-care/post-covid-c... Available. Accessed.
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous