

Analysis and prediction of contralateral central lymph node metastasis risk in unilateral papillary thyroid carcinoma with ipsilateral lateral cervical lymph node: a retrospective clinical study
- PMID: 40256465
- PMCID: PMC12004314
- DOI: 10.21037/gs-24-473
Analysis and prediction of contralateral central lymph node metastasis risk in unilateral papillary thyroid carcinoma with ipsilateral lateral cervical lymph node: a retrospective clinical study
Abstract
Background: Papillary thyroid carcinoma (PTC) often metastasizes to lymph nodes, increasing recurrence risk and reducing survival. This study identifies predictors for contralateral central lymph node metastasis (Cont-CLNM) in unilateral PTC patients with ipsilateral lateral cervical lymph node metastasis (Ipsi-LLNM).
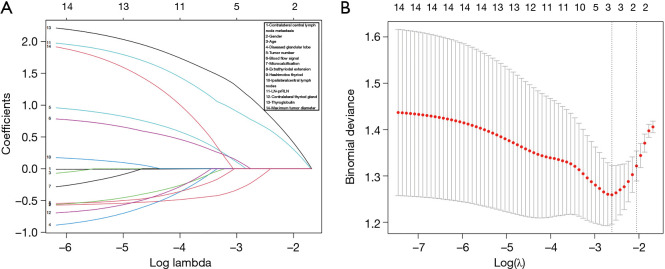
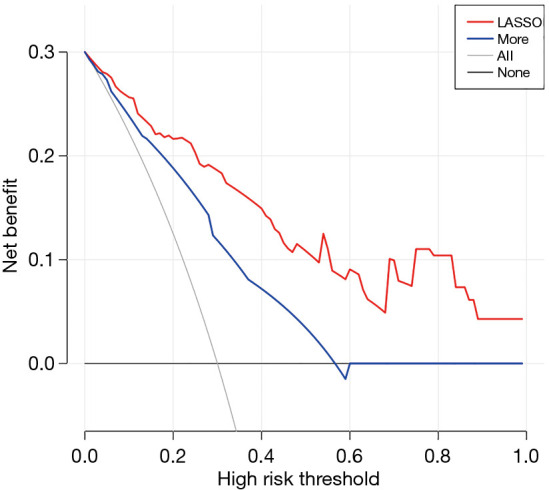
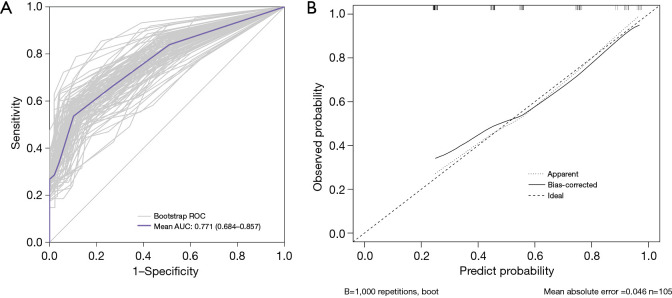
Methods: We retrospectively analyzed data, preoperative ultrasound features, and thyroglobulin (Tg) levels in unilateral PTC patients with Ipsi-LLNM treated at the Thyroid Surgery Department of Nanjing Drum Tower Hospital from August 2017 to August 2024. Least absolute shrinkage and selection operator (LASSO) regression was used for variable selection, with independent t-tests and Chi-squared tests assessing differences. Logistic regression analyses identified risk factors for Cont-CLNM, and a nomogram was validated using 1,000 bootstrap resamples. Decision curve analysis (DCA) evaluated clinical impact.
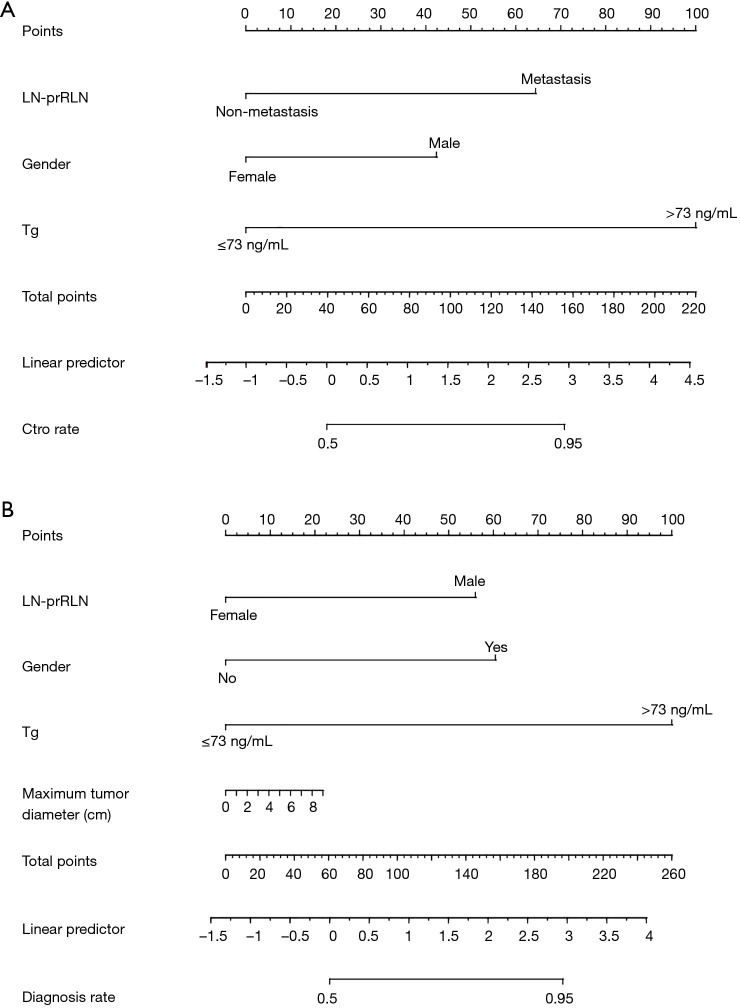
Results: Of 105 PTC patients, 56 (53.3%) had Cont-CLNM. LASSO regression identified three predictors: male sex, lymph node metastasis posterior to the recurrent laryngeal nerve (LN-prRLN), and elevated Tg levels. Multivariate regression confirmed these variables' association with Cont-CLNM. Internal validation yielded an area under the curve of 0.771 [95% confidence interval (CI): 0.684-0.857]. A nomogram was developed and validated through DCA.
Conclusions: Our findings indicate that combining male gender, LN-prRLN, and Tg levels effectively predicts Cont-CLNM, providing a basis for risk assessment in unilateral PTC.
Keywords: Papillary thyroid carcinoma (PTC); contralateral central lymph node metastasis (Cont-CLNM); ipsilateral lateral cervical lymph node metastasis (Ipsi-LLNM); predictive model; risk factors.
Copyright © 2025 AME Publishing Company. All rights reserved.
Conflict of interest statement
Conflicts of Interest: All authors have completed the ICMJE uniform disclosure form (available at https://gs.amegroups.com/article/view/10.21037/gs-24-473/coif). The authors have no conflicts of interest to declare.
Figures
Similar articles
-
[Risk factors for contralateral central lymph node metastasis in unilateral papillary thyroid carcinoma].Zhonghua Er Bi Yan Hou Tou Jing Wai Ke Za Zhi. 2025 May 7;60(5):505-510. doi: 10.3760/cma.j.cn115330-20250127-00079. Zhonghua Er Bi Yan Hou Tou Jing Wai Ke Za Zhi. 2025. PMID: 40419334 Chinese.
-
Nomogram model based on preoperative serum thyroglobulin and clinical characteristics of papillary thyroid carcinoma to predict cervical lymph node metastasis.Front Endocrinol (Lausanne). 2022 Jul 15;13:937049. doi: 10.3389/fendo.2022.937049. eCollection 2022. Front Endocrinol (Lausanne). 2022. PMID: 35909521 Free PMC article.
-
Constructing a nomogram based on the distribution of thyroid nodules and suspicious lateral cervical lymph nodes in fine-needle aspiration biopsies to predict metastasis in papillary thyroid carcinoma.Front Endocrinol (Lausanne). 2023 Nov 28;14:1242061. doi: 10.3389/fendo.2023.1242061. eCollection 2023. Front Endocrinol (Lausanne). 2023. PMID: 38089614 Free PMC article.
-
Analysis of Risk Factors and Risk Prediction for Cervical Lymph Node Metastasis in Thyroid Papillary Carcinoma.Cancer Manag Res. 2024 Nov 11;16:1571-1585. doi: 10.2147/CMAR.S485708. eCollection 2024. Cancer Manag Res. 2024. PMID: 39555445 Free PMC article.
-
Development and validation of a nomogram for preoperative prediction of ipsilateral cervical central lymph node metastasis in papillary thyroid cancer: a population-based study.Gland Surg. 2024 Apr 29;13(4):528-539. doi: 10.21037/gs-23-478. Epub 2024 Apr 22. Gland Surg. 2024. PMID: 38720676 Free PMC article.
References
-
- Sheng L, Shi J, Han B, et al. Predicting factors for central or lateral lymph node metastasis in conventional papillary thyroid microcarcinoma. Am J Surg 2020;220:334-40. - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous