

Identifying heterogeneity of treatment effect for antibiotic duration in bloodstream infection: an exploratory post-hoc analysis of the BALANCE randomised clinical trial
- PMID: 40256773
- PMCID: PMC12008128
- DOI: 10.1016/j.eclinm.2025.103195
Identifying heterogeneity of treatment effect for antibiotic duration in bloodstream infection: an exploratory post-hoc analysis of the BALANCE randomised clinical trial
Abstract
Background: The BALANCE trial demonstrated non-inferiority of 7 (vs 14) day antibiotic durations in patients with uncomplicated non-S. aureus/lugdunensis bacterial bloodstream infections (BSI). However, there may be patient subgroups who benefit from longer durations. We aimed to evaluate if bedside clinical decision rules could identify these subgroups.
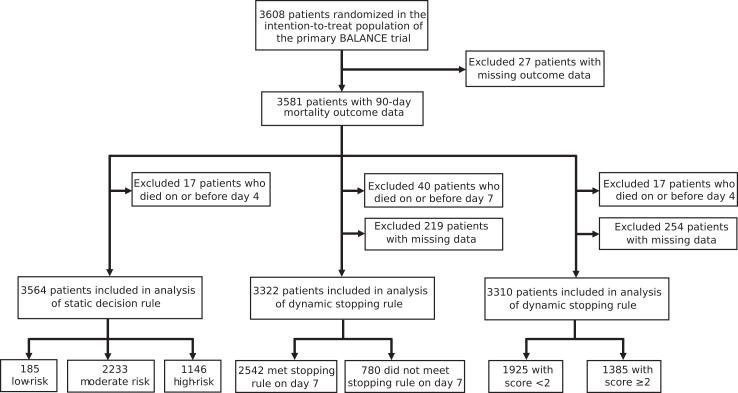
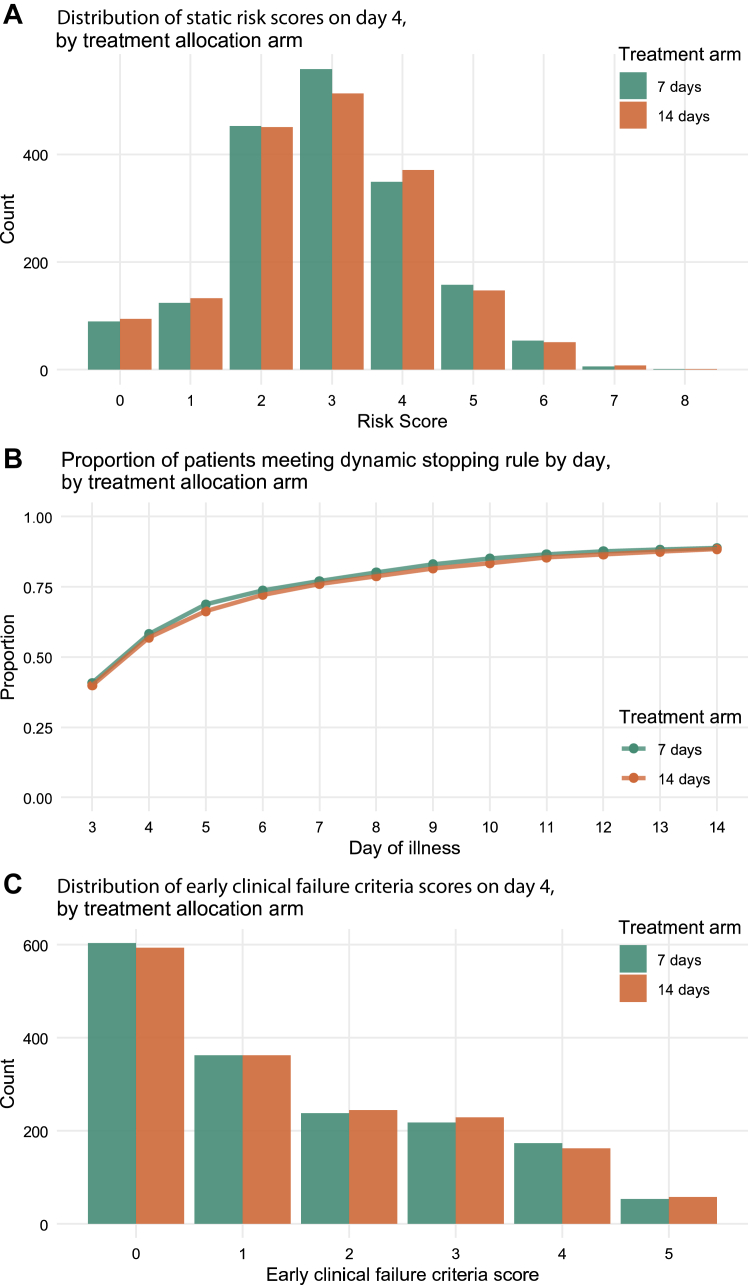
Methods: In this post-hoc analysis of the multicentre, randomised BALANCE trial (October 17, 2014-May 5, 2023), we applied three clinical decision rules to investigate heterogeneity of treatment effect in 7-day vs 14-day antibiotic durations on 90-day all-cause mortality. We used the rules to categorize patients in BALANCE into different risk groups and calculated the unadjusted absolute risk difference (RD) for 90-day mortality in patients receiving 7- vs 14-day antibiotics within each risk group. Statistical significance was tested using an interaction test. The BALANCE trial is registered with ClinicalTrials.gov (NCT03005145).
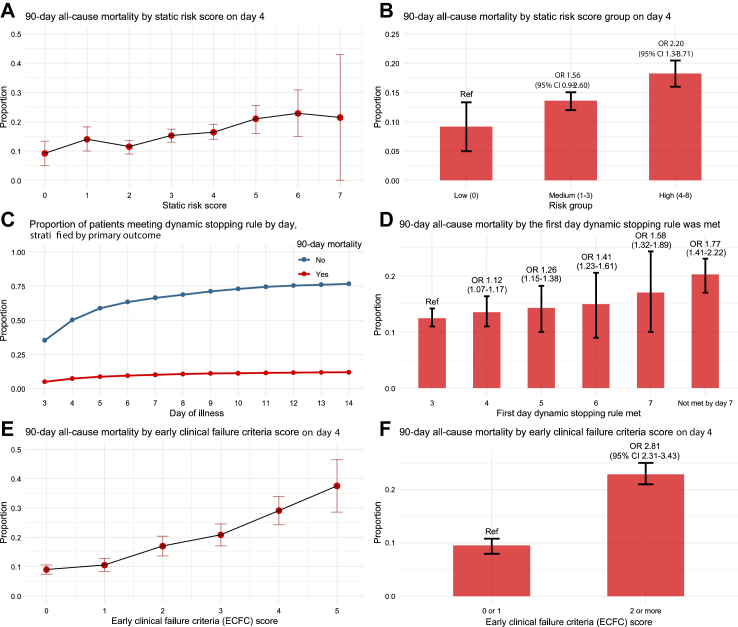
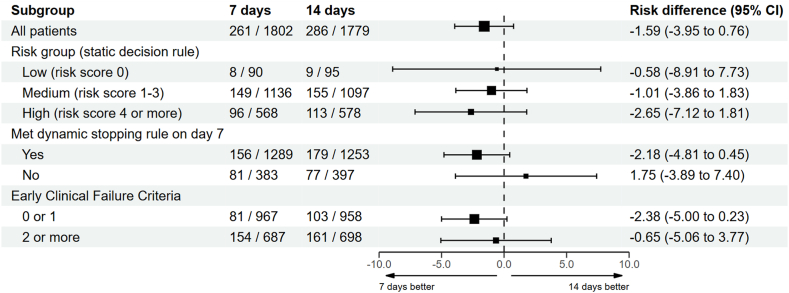
Findings: 3581 patients were included. All three rules predicted mortality risk, but none identified statistically significant effect modification: (a) static rule (low-risk: RD -0.58, 95% CI -8.91 to 7.73; moderate-risk: RD -.01, 95% CI -3.86 to 1.83; high-risk: RD -2.65, 95% CI -7.12 to 1.81; p = 0.74); (b) dynamic rule (met rule on day 7: RD -2.18, 95% CI -4.81 to 0.45; did not meet rule: RD 1.75, 95% CI -3.89 to 7.40; p = 0.16); and (c) early clinical failure criteria (score<2: RD -2.38, 95% CI -5.0 to 0.23; score ≥2: RD -0.65, 95% CI -5.06 to 3.77; p = 0.24). Results were consistent across sensitivity analyses including imputation for missing data and restricting analyses to gram-negative BSI.
Interpretation: The decision rules included in our analyses did not identify a subgroup of patients within BALANCE that would benefit from 14 (vs 7) days of treatment. 7-day treatment duration is sufficient for most patients with uncomplicated non-S. aureus/lugdunensis BSI. Future research could explore data-driven machine-learning approaches to identify comprehensive combinations of patient characteristics that may guide individualised duration of antibiotic therapy.
Funding: The BALANCE trial was funded by the Canadian Institutes of Health Research, Health Research Council of New Zealand, Australian National Medical Research Council, Physicians Services Incorporated Ontario and Ontario Ministry of Health and Long-term Care Innovation Fund. SWXO conducted this study as part of his PhD studies, with funding from: the Emerging & Pandemic Infections Consortium (University of Toronto, Canada); Connaught International Scholarship (University of Toronto, Canada); the Queen Elizabeth II Graduate Scholarship in Science and Technology (QEII-GSST; Government of Ontario, Canada); and the Melbourne Research Scholarship (University of Melbourne, Australia). VML is supported by Clinical Research Scholar-Junior 2 program (FRQ-S).
Keywords: Antibiotic duration; Antimicrobial stewardship; Bloodstream infections; Clinical trial; Heterogeneity of treatment effect.
© 2025 The Author(s).
Conflict of interest statement
JMC declares accommodations and airfare to attend and speak at a symposium in 2022 from bioMerieux Canada on antimicrobial resistance co-hosted by the University of Toronto and bioMerieux Canada in 2022, and accommodations and airfare from the 2023 ICPIC meeting to attend a Think Tank meeting on infectious diseases modelling in Geneva, Switzerland. MF was a paid consultant for ProofDx, a start-up company creating a point-of-care device for COVID-19 using CRISPR. MF is an advisor to SIGNAL1, a start-up company that implements machine-learned solutions into clinical practice, and declares stock options with this company. MF declares personal payments as an expert witness on content unrelated to this work, and payments to his institution as part of the Canadian Institutes of Health Research Project Grant (PJT 148749) related to this work. TCL declares research salary support from Fonds du Recherche Quebec—Sante; and operating grants from the Canadian Institutes of Health Research, including for the conduct of the original BALANCE trial. DY declares funding to her institution from Pfizer for a collaborative retrospective study, and funding to her institution from Shionogi for an investigator-initiated clinical study studying cefiderocol. VML declares research salary support from Fonds du Recherche Quebec—Sante and grant payments to her institution from Gilead Sciences. RAF declares receipt of a peer-reviewed grant from Canadian Institutes of Health Research. All other authors declare no competing interests.
Figures
References
-
- Spellberg B., Rice L.B. The shorter is better movement: past, present, future. Clin Microbiol Infect. 2022;29(2):141–142. - PubMed
-
- BALANCE Investigators, for the Canadian Critical Care Trials Group, the Association of Medical Microbiology and Infectious Disease Canada Clinical Research Network, the Australian and New Zealand Intensive Care Society Clinical Trials Group, and the Australasian Society for Infectious Diseases Clinical Research Network. Daneman N., Rishu A., et al. Antibiotic treatment for 7 versus 14 Days in patients with bloodstream infections. N Engl J Med. 2025;392(11):1065–1078. - PubMed
-
- Wang R., Lagakos S.W., Ware J.H., Hunter D.J., Drazen J.M. Statistics in medicine--reporting of subgroup analyses in clinical trials. N Engl J Med. 2007;357(21):2189–2194. - PubMed
-
- Cui L., Hung H.M., Wang S.J., Tsong Y. Issues related to subgroup analysis in clinical trials. J Biopharm Stat. 2002;12(3):347–358. - PubMed
-
- Brookes S.T., Whitely E., Egger M., Smith G.D., Mulheran P.A., Peters T.J. Subgroup analyses in randomized trials: risks of subgroup-specific analyses; power and sample size for the interaction test. J Clin Epidemiol. 2004;57(3):229–236. - PubMed
Associated data
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
