

Endoscopic diagnosis of immunoglobulin G4-related sclerosing cholangitis
- PMID: 40256978
- PMCID: PMC12333321
- DOI: 10.1111/den.15039
Endoscopic diagnosis of immunoglobulin G4-related sclerosing cholangitis
Abstract
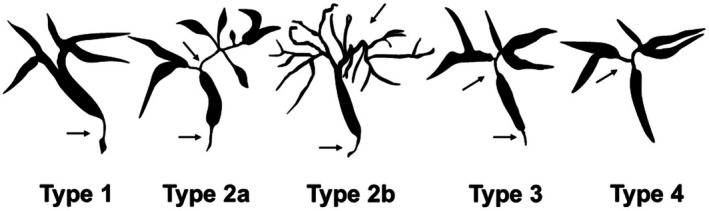
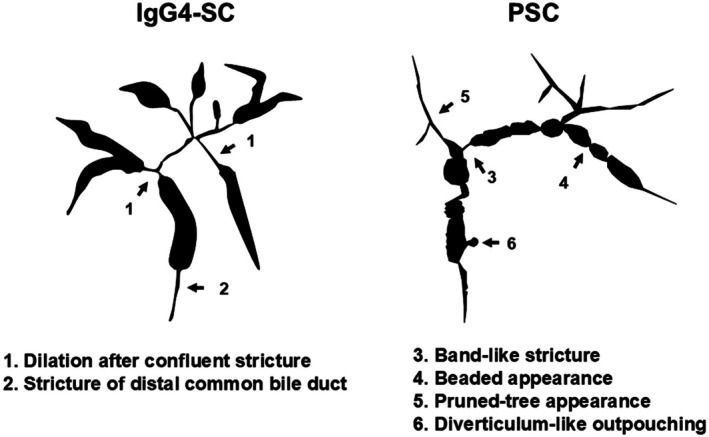
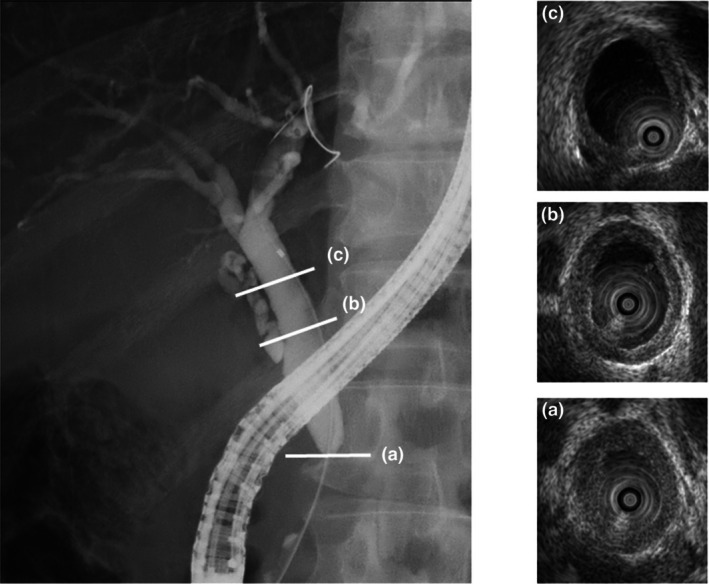
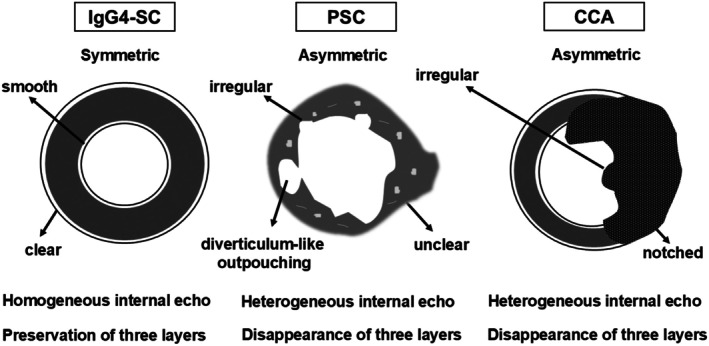
Immunoglobulin G4 (IgG4)-related sclerosing cholangitis (IgG4-SC) is a distinct form of sclerosing cholangitis frequently associated with autoimmune pancreatitis and is recognized as a biliary manifestation of IgG4-related disease. Endoscopic retrograde cholangiopancreatography (ERCP) and endoscopic ultrasonography (EUS) are key diagnostic modalities for IgG4-SC. Cholangiocarcinoma and primary sclerosing cholangitis (PSC) are significant mimickers of IgG4-SC. ERCP is employed to evaluate narrowing of the bile duct, with cholangiograms of IgG4-SC classified into four types. This cholangiographic classification is crucial for differential diagnosis. Characteristic cholangiographic findings of IgG4-SC include diffuse or segmental strictures of the intrahepatic or extrahepatic bile ducts and intrahepatic strictures associated with autoimmune pancreatitis. ERCP is particularly useful for differentiating IgG4-SC from PSC because their cholangiographic features differ. EUS and intraductal ultrasonography (IDUS) are used to assess thickening of the bile duct wall. Characteristic IDUS findings in IgG4-SC include circular and symmetrical wall thickening, smooth outer and inner margins, and homogeneous internal echoes at stricture sites. Additionally, bile duct wall thickening at nonstricture sites is a typical IDUS feature of IgG4-SC. Bile duct biopsy is used to evaluate pathological findings, although its diagnostic yield for IgG4-SC is limited; its primary role is to exclude malignant biliary strictures. Duodenal papilla biopsy serves as a supplementary diagnostic tool for IgG4-SC. EUS and tissue acquisition also aid in diagnosing autoimmune pancreatitis as part of other organ involvement. Thus, endoscopic techniques play critical roles in the diagnosis of IgG4-SC.
Keywords: IgG4‐related sclerosing cholangitis; autoimmune pancreatitis; endoscopic retrograde cholangiopancreatography; endoscopic ultrasonography; intraductal ultrasonography.
© 2025 The Author(s). Digestive Endoscopy published by John Wiley & Sons Australia, Ltd on behalf of Japan Gastroenterological Endoscopy Society.
Conflict of interest statement
Authors declare no conflict of interest for this article.
Figures
Similar articles
-
Endoscopic retrograde cholangiopancreatography and intraductal ultrasonography in the diagnosis of autoimmune pancreatitis and IgG4-related sclerosing cholangitis.J Med Ultrason (2001). 2021 Oct;48(4):573-580. doi: 10.1007/s10396-021-01114-1. Epub 2021 Jul 31. J Med Ultrason (2001). 2021. PMID: 34331625 Review.
-
Endoscopic management of primary sclerosing cholangitis.Dig Endosc. 2025 Jul;37(7):723-732. doi: 10.1111/den.15010. Epub 2025 Mar 6. Dig Endosc. 2025. PMID: 40049717 Free PMC article. Review.
-
Role of endoscopy in the diagnosis of autoimmune pancreatitis and immunoglobulin G4-related sclerosing cholangitis.Dig Endosc. 2014 Sep;26(5):627-35. doi: 10.1111/den.12289. Epub 2014 Apr 8. Dig Endosc. 2014. PMID: 24712522 Review.
-
Endoscopic transpapillary intraductal ultrasonography and biopsy in the diagnosis of IgG4-related sclerosing cholangitis.J Gastroenterol. 2009;44(11):1147-55. doi: 10.1007/s00535-009-0108-9. Epub 2009 Jul 28. J Gastroenterol. 2009. PMID: 19636664
-
Usefulness of laparoscopy and intraductal ultrasonography in a patient with isolated immunoglobulin G4-related sclerosing cholangitis.Clin J Gastroenterol. 2018 Feb;11(1):62-68. doi: 10.1007/s12328-017-0787-3. Epub 2017 Nov 1. Clin J Gastroenterol. 2018. PMID: 29094322
References
-
- Ohara H, Okazaki K, Tsubouchi H et al. Clinical diagnostic criteria of IgG4‐related sclerosing cholangitis 2012. J Hepatobiliary Pancreat Sci 2012; 19: 536–542. - PubMed
-
- Nakazawa T, Kamisawa T, Okazaki K et al. Clinical diagnostic criteria for IgG4‐related sclerosing cholangitis 2020: (Revision of the clinical diagnostic criteria for IgG4‐related sclerosing cholangitis 2012). J Hepatobiliary Pancreat Sci 2021; 28: 235–242. - PubMed
-
- Madhusudhan KS, Das P, Gunjan D, Srivastava DN, Garg PK. IgG4‐related sclerosing cholangitis: A clinical and imaging review. AJR Am J Roentgenol 2019; 213: 1221–1231. - PubMed
-
- Kersten R, Trampert DC, Herta T et al. IgG4‐related cholangitis – a mimicker of fibrosing and malignant cholangiopathies. J Hepatol 2023; 79: 1502–1523. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
