

Low risk for locally acquired Chagas disease in California: A review of human cases and triatomine submissions, 2013-2023
- PMID: 40258046
- PMCID: PMC12043235
- DOI: 10.1371/journal.pntd.0013036
Low risk for locally acquired Chagas disease in California: A review of human cases and triatomine submissions, 2013-2023
Abstract
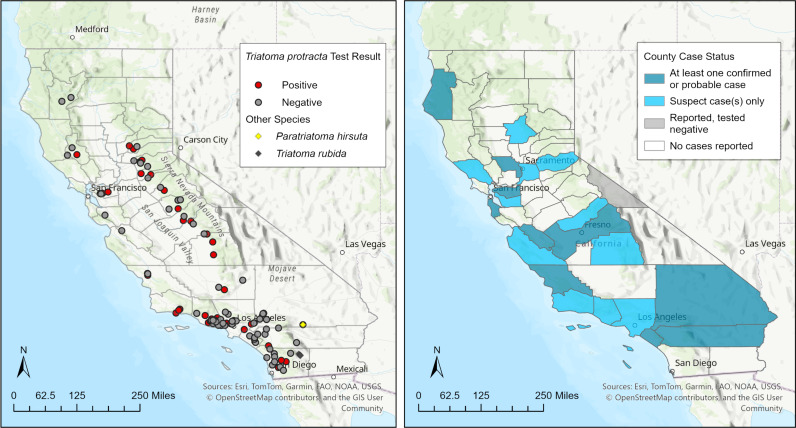
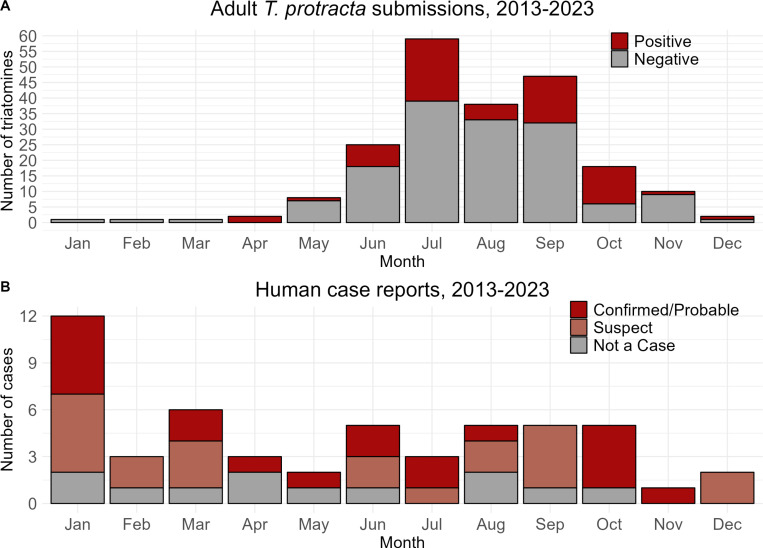
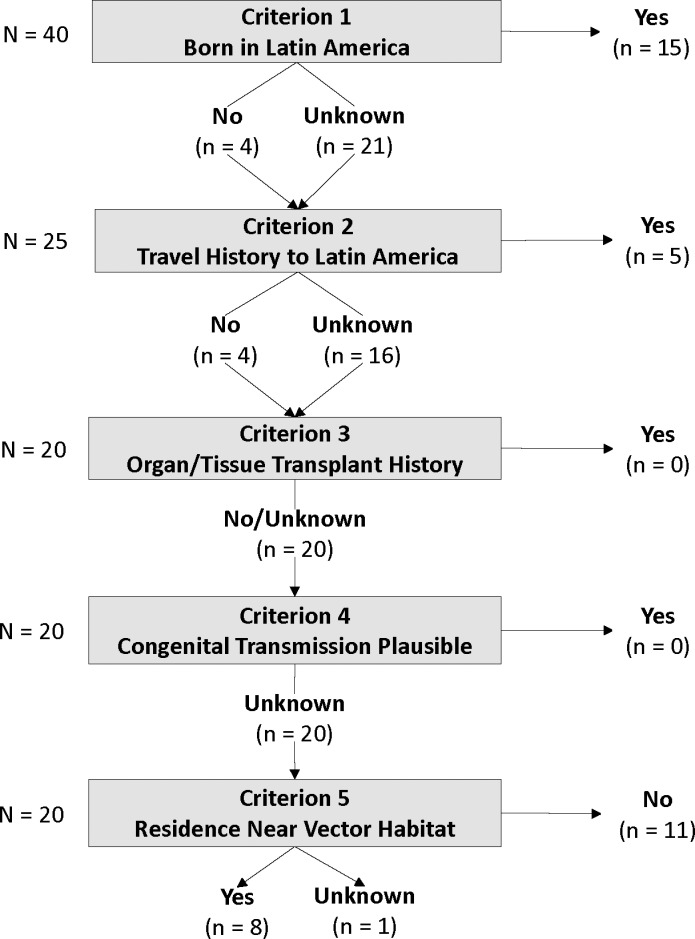
Chagas disease is caused by infection with the protozoan parasite Trypanosoma cruzi, which is carried in the guts of triatomine insects. Transmission typically occurs when infective trypomastigotes in triatomine feces encounter mucous membranes or bite wounds, though it is also possible by food-borne, transplant- and transfusion-mediated, and congenital routes. Most transmission occurs in rural and peri-urban parts of continental Latin America where triatomines often inhabit human dwellings. Triatomines infected with T. cruzi are also present across the southern United States, yet relatively few locally acquired infections have been documented. Rather, most reported cases have plausible exposure in Latin America. In California, the widespread distribution of T. cruzi-infected triatomines suggests a potential risk of local transmission. Here, we summarize triatomine submissions and human case reports made to the California Department of Public Health between 2013 and 2023. Of 226 triatomines tested, 63 (28%) were positive for T. cruzi via PCR; none were linked to any of the 40 human T. cruzi cases reported in the same period. Human cases were assessed for likelihood of local transmission. Country of birth, travel history, and location of primary residence suggested non-local transmission for 31 (78%) cases. Local transmission could not be ruled out for the remaining nine (22%) cases. Information on country of birth and travel history were missing from these case reports and prevented full assessment of local transmission criteria, though most of these patients resided within 400 meters of potential triatomine habitat. Despite the presence of triatomines, T. cruzi, and human cases in California, statewide data indicates the risk for locally acquired Chagas disease is low.
Copyright: © 2025 Lund et al. This is an open access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
Similar articles
-
Detection of Trypanosoma cruzi strains circulating in Córdoba department (Colombia) isolated from triatomines (Hemiptera: Reduviidae) collected by the community.Biomedica. 2019 Jun 15;39(2):265-277. doi: 10.7705/biomedica.v39i2.3973. Biomedica. 2019. PMID: 31529814 English, Spanish.
-
Panstrongylus geniculatus and four other species of triatomine bug involved in the Trypanosoma cruzi enzootic cycle: high risk factors for Chagas' disease transmission in the Metropolitan District of Caracas, Venezuela.Parasit Vectors. 2014 Dec 23;7:602. doi: 10.1186/s13071-014-0602-7. Parasit Vectors. 2014. PMID: 25532708 Free PMC article.
-
The potential risk of enzootic Trypanosoma cruzi transmission inside four training and re-training military battalions (BITER) in Colombia.Parasit Vectors. 2021 Oct 9;14(1):519. doi: 10.1186/s13071-021-05018-4. Parasit Vectors. 2021. PMID: 34625109 Free PMC article.
-
History of indigenous Trypanosoma cruzi infection in humans, animals and triatomines in California, USA.Zoonoses Public Health. 2021 Jun;68(4):299-308. doi: 10.1111/zph.12797. Epub 2020 Dec 31. Zoonoses Public Health. 2021. PMID: 33382207 Review.
-
Triatomines: Trypanosomatids, Bacteria, and Viruses Potential Vectors?Front Cell Infect Microbiol. 2018 Nov 16;8:405. doi: 10.3389/fcimb.2018.00405. eCollection 2018. Front Cell Infect Microbiol. 2018. PMID: 30505806 Free PMC article. Review.
Cited by
-
Characterizing the transmission dynamics of Trypanosoma cruzi in Triatoma sanguisuga collected from dog kennels in southern Texas.Parasit Vectors. 2025 Jul 15;18(1):284. doi: 10.1186/s13071-025-06917-6. Parasit Vectors. 2025. PMID: 40665373 Free PMC article.
References
-
- Ryckman RE, Folkes DL, Olsen LE, Robb PL, Ryckman AE. Epizootiology of Trypanosoma cruzi in southwestern North America. J Med Entomol. 1965; 2. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
