

Pharmacokinetics of metal excretion following different doses of sodium EDTA infusion
- PMID: 40258339
- PMCID: PMC12050972
- DOI: 10.1093/mtomcs/mfaf010
Pharmacokinetics of metal excretion following different doses of sodium EDTA infusion
Abstract
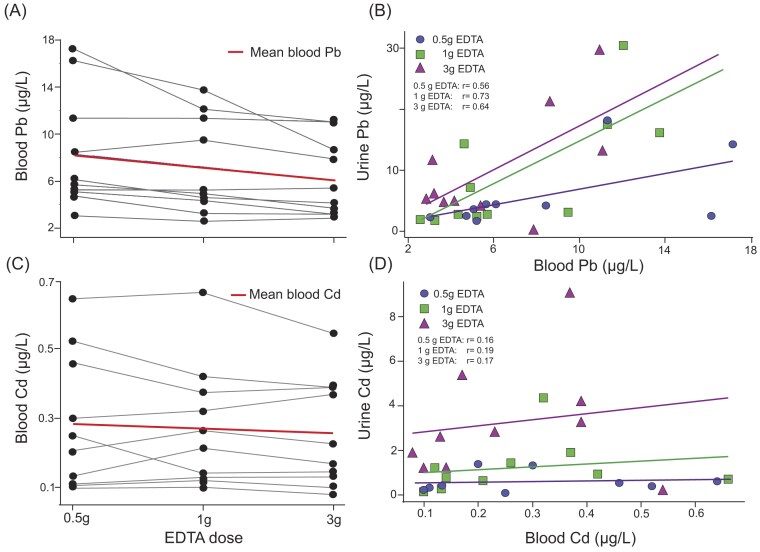
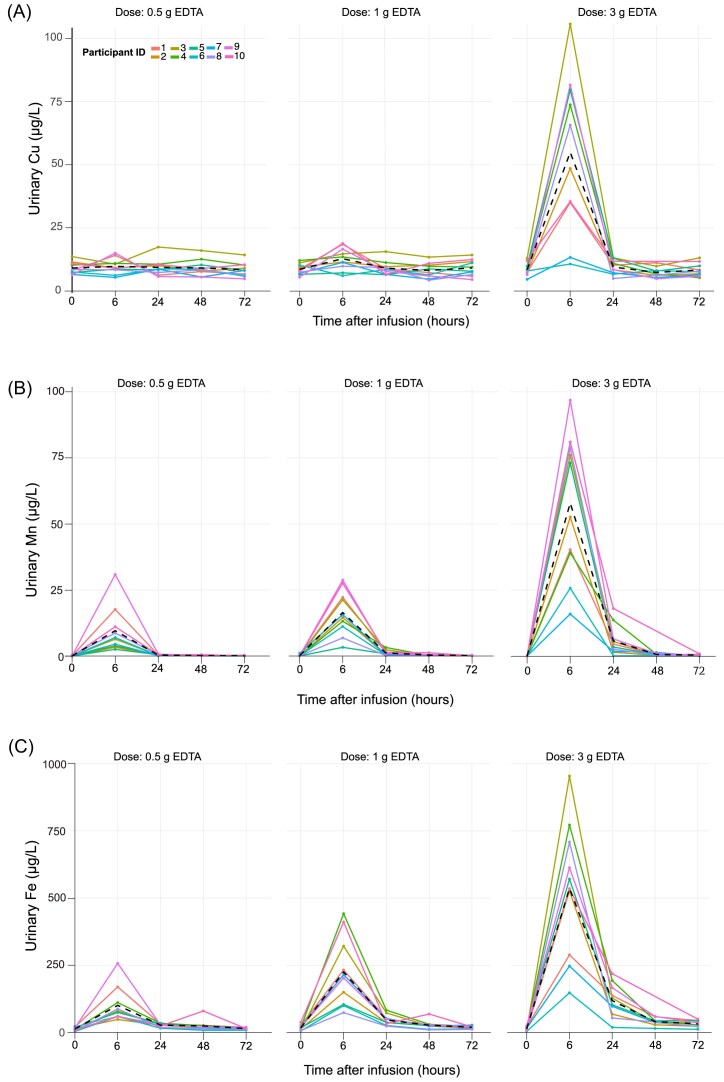
Chelation therapy is a promising approach to mitigating health risks associated with toxic metal exposure, which contributes to cardiovascular disease, neurotoxicity, and other chronic conditions. disodium ethylene diamine tetraacetic acid (EDTA) is widely used, but its optimal dosing strategy remains unclear. This study evaluates the dose-dependent efficacy of EDTA in mobilizing toxic metals, including lead (Pb), cadmium (Cd), and gadolinium (Gd), while minimizing the loss of essential metals like copper (Cu) and manganese (Mn) to optimize therapeutic safety and efficacy. Ten volunteers (≥50 years) received 3 infusions at doses of 0.5, 1, and 3 g of EDTA over 30 min, 1 h, and 3 h, respectively. Urine and blood samples were analyzed pre- and post-infusion to assess pharmacokinetics of metal chelation. Urinary Pb excretion increased by 2200% at 0.5 g, with only a marginal gain at higher doses (3300%), supporting low-dose EDTA efficacy. Urinary Cd clearance required 3 g EDTA due to its strong tissue binding. Notably, Gd excretion increased by up to 78 000% even at 0.5 g EDTA, highlighting EDTA's potential to reduce long-term Gd burden post-MRI. Urinary excretion of essential metals varied, with Mn and Zn loss increasing at higher EDTA doses, underscoring the need for dose optimization while Cu and Ca only showed a clear increase urinary excretion at 3 g EDTA. Overall, a 0.5 g EDTA dose effectively mobilized Pb and Gd while minimizing essential metal depletion, reducing infusion time to 30 min, and improving patient compliance. These findings align with TACT and TACT 2 studies, reinforcing EDTA's long-term benefits in Pb reduction and supporting low-dose EDTA as a safe, efficient, and well-tolerated detoxification strategy.
© The Author(s) 2025. Published by Oxford University Press.
Conflict of interest statement
None declared.
Figures







References
-
- Lamas GA, Bhatnagar A, Jones MR et al. American Heart Association Council on Epidemiology and Prevention; Council on Cardiovascular and Stroke Nursing; Council on Lifestyle and Cardiometabolic Health; Council on Peripheral Vascular Disease; and Council on the Kidney in Cardiovascular Disease. Contaminant Metals as Cardiovascular Risk Factors: A Scientific Statement From the American Heart Association. J Am Heart Assoc. 2023;12:e029852. - PMC - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
